Location: Home >> Detail
Adv Geriatr Med Res. 2020;2(4):e200021. https://doi.org/10.20900/agmr20200021
 ,
François Béland 3,4,5,
Claude Galand 5,
John D. Fletcher 5,
Joel Tuakuila 2,
Marie-Pierre Garant 6
,
François Béland 3,4,5,
Claude Galand 5,
John D. Fletcher 5,
Joel Tuakuila 2,
Marie-Pierre Garant 6
1 École de réadaptation, Faculté de médecine et des sciences de la santé, Université de Sherbrooke, J1H 5N4 Québec, Canada
2 Research Center on Aging, Sherbrooke, J1H 4C4, Québec, Canada
3 École de santé publique, Département d'administration de la santé, Université de Montréal, H3N 1X9 Québec, Canada
4 Faculty of Medicine, McGill University, Jewish General Hospital, Montreal, H3T 1E2 Québec, Canada
5 McGill University-University of Montreal Research Group on Frailty and Aging (SOLIDAGE), Montreal, H3T 1E2 Québec, Canada
6 Research Center, Centre hospitalier universitaire de Sherbrooke, Sherbrooke, J1H 5H3 Québec, Canada
* Correspondence: Véronique Provencher.
Only 4–7% of people aged 65–74 are considered frail. However, this youngest-old subgroup may live for several decades with chronic diseases and reduced quality of life. Therefore, it is essential to identify how life-course factors contribute to the manifestation of individual frailty components in order to design interventions that could prevent or mitigate their adverse effects in community-dwelling youngest-old. This study explored whether lifestyle habits (tobacco/alcohol consumption, sleep quality), geographic location (metropolitan/urban/semi-rural), and type of work increase the risk of exhibiting frailty components at a younger age. Using a cross-sectional design involving 1643 community-dwelling older adults (65+), logistic regression models showed that current but not past smoking was strongly related to low physical activity earlier in life (OR: 3.08; CI: 1.12–8.44). Lifetime number of cigarettes smoked also significantly increased the risk of exhibiting this frailty component in the youngest-old subgroup only. Poor sleep contributed to another frailty component (exhaustion) (OR: 2.52; CI: 1.46–4.37), while moderate alcohol consumption was a protective factor against three frailty components. However, these relationships were not found exclusively in the youngest-old. Living in an urban area was the only factor that contributed significantly less to individual frailty components (slowness) with advancing age, when compared to semi-rural areas. This study expands on previous work by exploring the contribution of life-course factors pertaining to lifestyle, geographic location and type of work to the manifestation of specific frailty components in the youngest-old. Our findings may support the adaptation of public policy programs (e.g., stop smoking program for young older adults) to prevent the early manifestation of frailty.
Frail older adults are at increased risk of disability, hospitalization and institutionalization [1–4]. They often exhibit a combination of the following components: involuntary weight loss, decreased walking speed, muscle weakness, fatigue and low physical activity [2]. A conceptual model of frailty [5] suggested that life-course factors, such as lifestyle habits and living environments, contribute to a decline in physiological reserves which, combined with health problems, may lead to the manifestation of frailty, sometimes early in the aging process. Although only 4% to 7% of people aged 65 to 74 are considered “frail” [6–8], this youngest-old subgroup may live for several decades with chronic diseases, leading them to become major consumers of health services, and with reduced quality of life [6,9–11]. Because frailty is a potentially reversible state [12], there is a need to act upstream, even in the youngest-old. Based on the above model of frailty as well as theories of healthy aging using a life-course approach [13], there is reason to believe that the frail oldest-old, compared to the youngest-old, have physiological reserves that helped them cope with health problems earlier in life. Their ability to survive for a longer time may further suggest that different life-course factors contribute to frailty in different age groups. A better understanding of these factors, especially those that could be modified, may help to prevent or at least delay the early manifestation of frailty components in the youngest-old and potentially reduce the risk of adverse outcomes later in life.
The body of knowledge about how modifiable life-course factors, such as lifestyle habits, may contribute to frailty has been growing in recent years. Systematic reviews found that, throughout the aging process, frailty was associated with smoking [14] and sleep disorders [15] while, surprisingly, high alcohol consumption has been reported to have a protective effect [16]. However, recent studies did not reach similar conclusions as they did not find a significant relationship between frailty and smoking [17] or suggest that heavy drinkers are at higher risk of frailty [18]. Moreover, the contribution of other life-course factors to frailty such as geographic location and type of work remains unclear. A few studies maintained that living in a rural area and being a blue-collar worker during one’s active life may be associated with frailty [19,20], but others did not support this conclusion [21,22]. It has been suggested that the discrepancy in these findings may be attributable to a lack of control over potential confounders and the way variables were measured. However, because little is known about the contribution of lifestyle habits, geographic location and type of work to the manifestation of frailty in the youngest-old in particular, we hypothesized that analyzing the data to identify differences between age groups might also shed light on these mixed results.
The lack of agreement between previous studies may also be related to differences in how current or past lifestyle, geographic location and type of work affect individual components of frailty. For example, it is possible that hard physical work (e.g., farmer) has a positive effect on grip strength [23] but induces more fatigue with aging. Similarly, descriptive data from a Korean study [24] indicated that rural older adults were less physically active, while those living in urban areas tended to show weight loss more often. Therefore, different programs (exercise or nutritional) designed to reduce frailty components may be offered to subgroups of older adults, according to where they live.
Furthermore, to our knowledge, the question of whether the relative contribution to frailty of each of these factors decreases with age has not been explored. For example, smoking—a risk factor for premature death [25] could be expected to contribute less to frailty over time. It is thus essential to identify how life-course factors contribute to the manifestation of frailty components in the youngest-old in order to design interventions that could prevent or mitigate their adverse effects. This knowledge could guide future public health policies and help to reduce the economic burden of care in an understudied subgroup of frail older adults.
This study aimed to evaluate the contribution of (a) lifestyle habits (tobacco and alcohol consumption, quality of sleep), (b) geographic location (semi-rural, urban or metropolitan area), and (c) type of work to the manifestation of individual frailty components in community-dwelling youngest-old (65–74 years). More specifically, we explored, first, (1) which of these potential life-course factors increase the risk of exhibiting components of frailty at a younger age, after controlling for confounders; and second, (2) whether the contribution of these possible life-course risk factors decreases with advancing age.
This cross-sectional study used data from the first wave of a multicenter longitudinal panel study called FRéLE. The FRéLE sample (n = 1643) consists of community-dwelling men and women aged 65 years and older living in the province of Québec, Canada. Participants were recruited from three different areas: metropolitan (Montreal), urban (Sherbrooke) and semi-rural (Victoriaville). They were randomly selected from a list generated by the Québec health insurance board (Régie de l’assurance-maladie du Québec). To be included, participants had to be able to answer the interview questions and be fluent in French or English. Exclusion criteria were (1) being hospitalized or living in a nursing home, or (2) exhibiting significant hearing impairments. Six strata (men and women in three age groups: 65–74; 75–84; 85+), each composed of at least 270 participants, were created. Details of the recruitment process and sample size calculation have been published elsewhere [26,27]. The research protocol was approved by the Jewish General Hospital Research Ethics Committee (05-2019-1457) and informed consent was obtained from all participants.
Questions pertaining to the following independent variables were taken from the National Population Health Survey questionnaire [28].
(1)
(2)
(3)
(4)
(5)
Frailty components were assessed using cutoff points to identify vulnerable respondents based on a five-component phenotype of frailty, i.e., weight loss, exhaustion, low physical activity, slowness, and weakness.
(1)
(2)
(3)
(4)
(5)
Control variables. Control variables (gender, education, income and comorbidity) were selected because of their potential impact on frailty [19,34–36] and according to other life-course factors included in the conceptual model of frailty [5]. Comorbidities were self-reported and measured using the Functional Comorbidity Index (FCI) [37] (comprising 18 diagnoses). Scores were recoded into three categories (0–1, 2–4, 5+ chronic diseases).
Descriptive analyses (frequency and percentage; mean and standard deviation) were conducted to describe the participants’ main characteristics. Survey analysis procedures (SAS version 9.4) were used to consider the survey sample design. Since dependent variables (individual frailty components) were binary (yes/no), logistic regression models were calculated to explore their relationship with each independent variable (selected life-course factors), by age group (65–74; 75–84; 85+) (objective 1). Univariate logistic regression analyses were first performed to reveal any unadjusted effect between the main variables. To adjust the effect for age, education, income and comorbidities, multivariate logistic regression models were then computed. For alcohol and tobacco consumption, further analyses were conducted to determine to what extent the type of drink, age at which the participant started drinking, and lifetime number of cigarettes smoked increased the risk of exhibiting frailty components.
Interaction effects were explored to determine whether the contribution of each life-course risk factor to frailty components decreases with advancing age by comparing the models created (OR) across age groups (65–74 vs 75–84 vs 85+) (objective 2).
Table 1 presents the main participants’ baseline characteristics. Frequencies were weighted to apply the results to the general population from which the participants were drawn. The proportion of women (57.8%) was slightly higher than that for men. The participants’ mean age was 75.4 years (SEM = 0.08) and more than one third reported living alone (35.2%). A majority (73.3%) of participants had completed a high school education degree (≥13 school years) and about one quarter (25.6%) reported a yearly income of $20,000 or less. Over half (52.1%) the participants reported 2 to 4 comorbidities. Based on the descriptive data, slowness was the most prevalent frailty component (20.0%), closely followed by exhaustion (19.2%). Almost half (47.6%) the participants were past smokers and a majority (59.2%) were moderate alcohol drinkers. Among drinkers, a large proportion reported consuming wine (64.8%) and, to a lesser extent, beer (43.3%) and hard liquor (24.8%); about a quarter of the sample (24.5%) started drinking before the age of 18. Nearly one quarter (22.4%) reported poor sleep. The majority of participants had been technicians or highly skilled workers (59.5%).
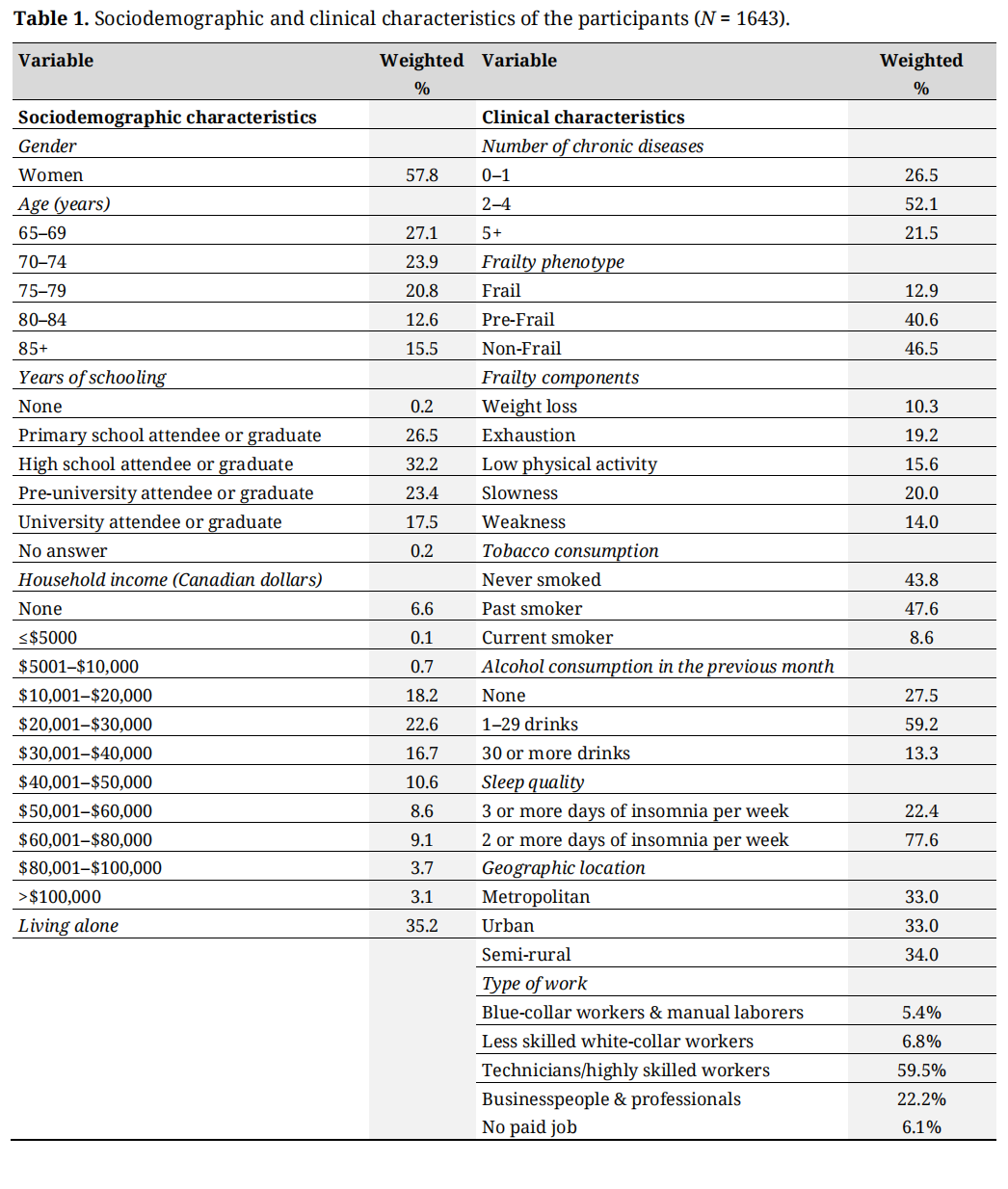 Table 1. Sociodemographic and clinical characteristics of the participants (N = 1643).
Table 1. Sociodemographic and clinical characteristics of the participants (N = 1643).
The main results for the youngest-old group from univariate and multivariate logistic regression analyses are presented in Tables 2–6. Univariate regression analysis revealed that living in an urban area was significantly associated (p = 0.036) with higher risk of slowness (OR: 2.31, CI: 1.06–5.08) compared to living in a semi-rural area. Unadjusted results also indicate that poorer sleep (3 or more nights of insomnia per week vs 2 or less) was significantly associated with exhaustion (p < 0.0001) and smoking (current vs never) with low physical activity (p = 0.026). These two relationships remained significant after adjusting for confounding variables (exhaustion: OR: 2.52, CI: 1.46–4.37; low physical activity: OR: 3.08, CI: 1.12–8.44). In other words, older adults with poor sleep were twice as likely to show exhaustion, while being a current smoker increased the risk of low physical activity by about 200%. However, the contribution of poor sleep to exhaustion was found across all age groups, while the relationship between current smoking and low physical activity disappeared in the oldest participants. Further analysis also confirmed a relationship between tobacco consumption and low physical activity in the youngest-old. More specifically, every 10,000 cigarettes smoked significantly increased the risk of exhibiting this frailty component in the subgroup (65–74: OR: 1.018; p < 0.01) but not in the other age groups (75–85: OR: 1.009, p = 0.11; 85+: OR: 1.007, p = 0.16). Interestingly, moderate alcohol consumption (1–29 drinks per month) was revealed to be a significant protective factor (p < 0.05) for all three of these frailty components (exhaustion: OR: 0.54, CI: 0.31–0.95; slowness: OR: 0.25, CI: 0.13–0.51; physical activity: OR: 0.44, CI: 0.22–0.87), as was high alcohol consumption (30+ drinks per month) in relation to low physical activity (OR: 0.20, CI: 0.05–0.76). Further analyses concerning the type of drink revealed that wine and, to a lesser extent, beer were significant protective factors for slowness (OR: 0. 573, p < 0.01; OR: 0.69, p = 0.049). Similarly, starting to drink later in life proved to be a protective factor for low physical activity since every year significantly reduced the risk of exhibiting this frailty component in the youngest-old only (OR: 0.906, p < 0.03). None of the contributing life-course factors studied were significantly associated with weight loss or grip strength at a younger age, except for hard liquor, which proved to be a risk factor for weakness in the youngest-old only (OR: 1.762, p < 0.01). Type of work (business & professional) was found to be significantly associated with some individual frailty components, but only in the oldest-old, showing a higher risk of weakness (OR: 2.905, p = 0.04) and lower risk of exhaustion (OR: 0.275, p = 0.03) compared to blue-collar & manual laborers. Detailed odds ratios (OR) and confidence intervals (95% CI) are shown for the main variables in Tables 2–6.
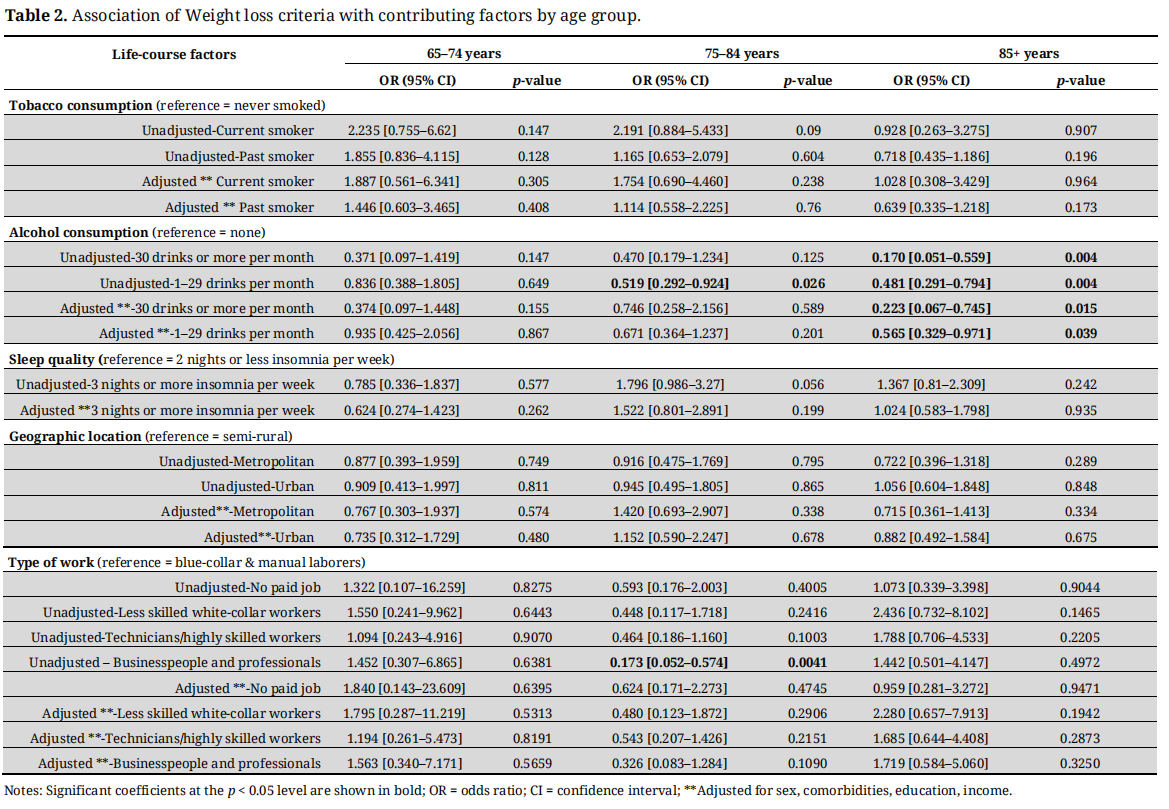 Table 2. Association of Weight loss criteria with contributing factors by age group.
Table 2. Association of Weight loss criteria with contributing factors by age group.
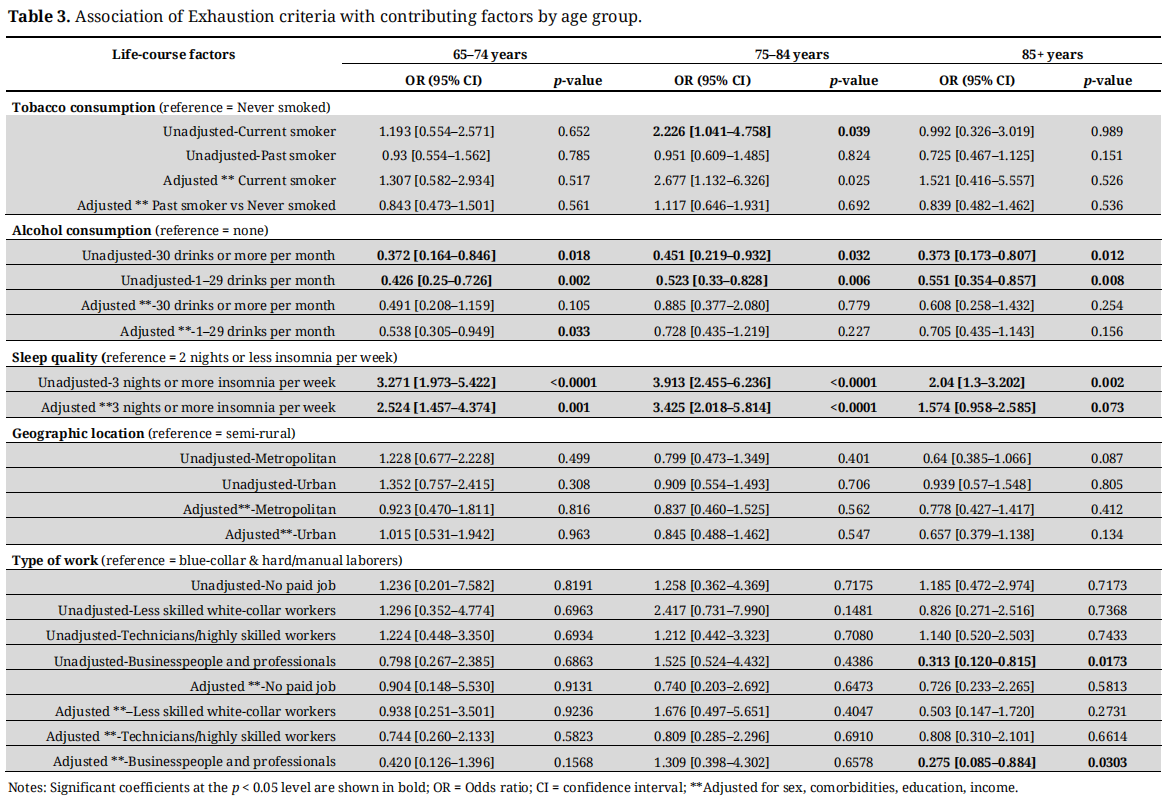 Table 3. Association of Exhaustion criteria with contributing factors by age group.
Table 3. Association of Exhaustion criteria with contributing factors by age group.
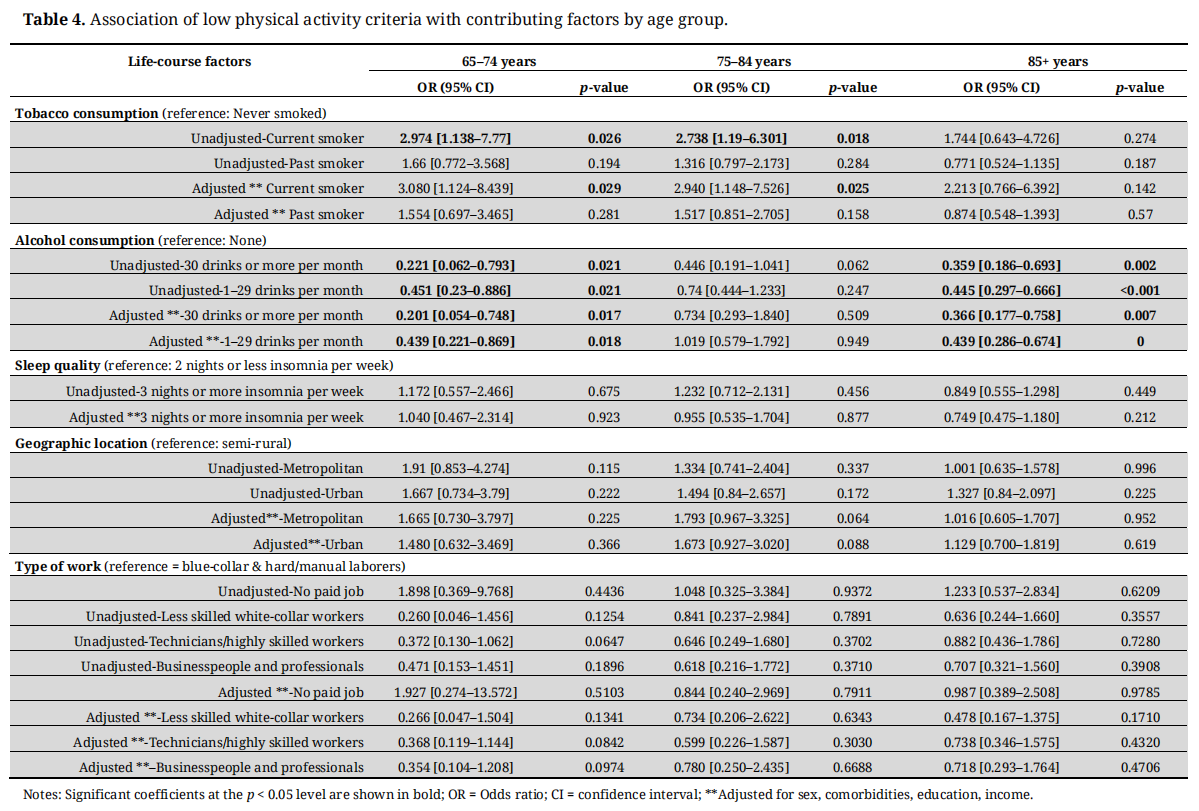 Table 4. Association of low physical activity criteria with contributing factors by age group.
Table 4. Association of low physical activity criteria with contributing factors by age group.
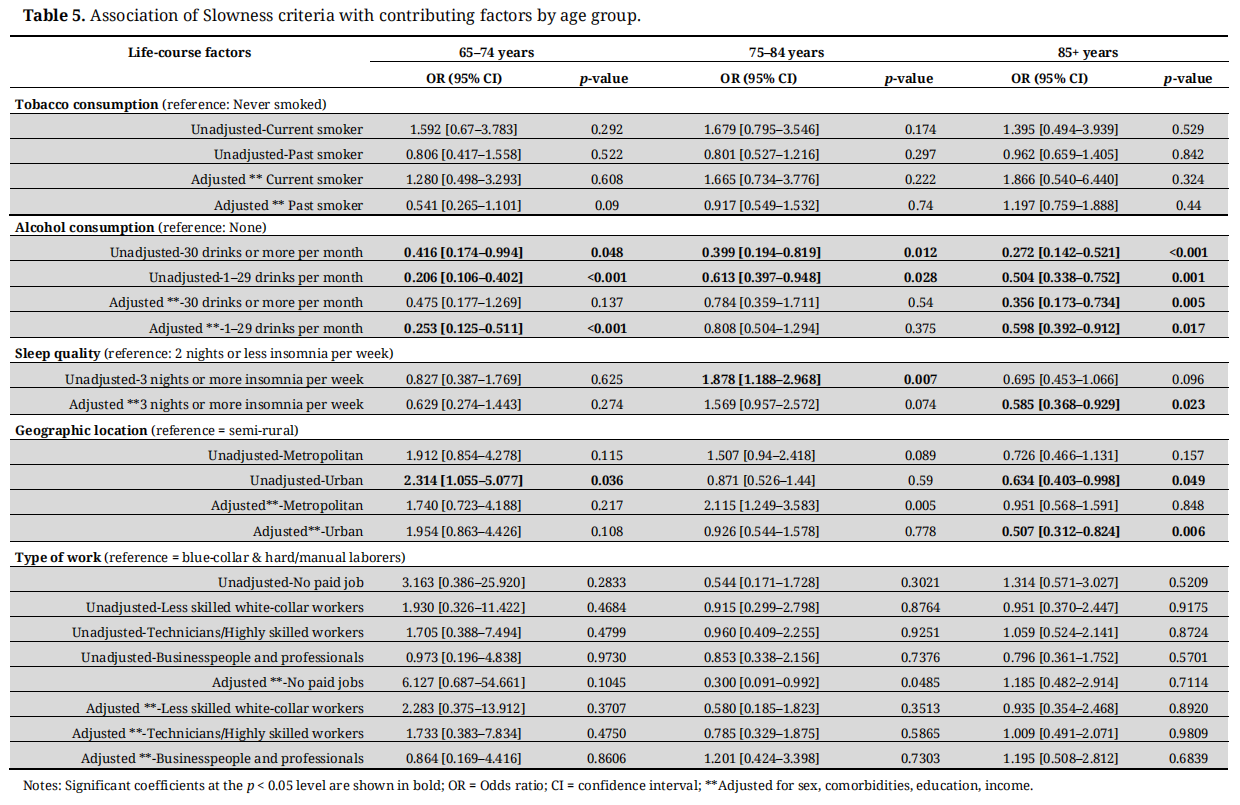 Table 5. Association of Slowness criteria with contributing factors by age group.
Table 5. Association of Slowness criteria with contributing factors by age group.
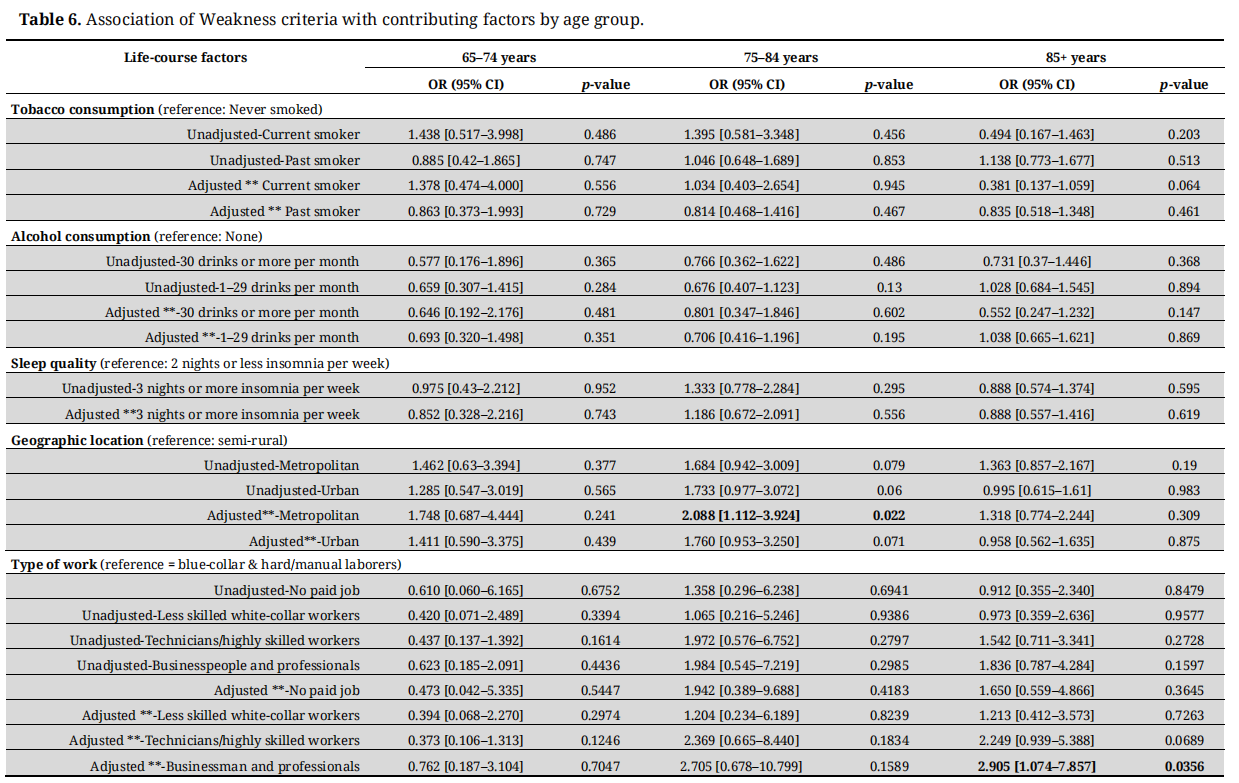 Table 6. Association of Weakness criteria with contributing factors by age group.
Table 6. Association of Weakness criteria with contributing factors by age group.
Our analyses also revealed that the interaction between geographic location and slowness was the only relationship that significantly decreased with age (p = 0.006) (see Table 5). This result suggested that living in an urban, as compared to a semi-rural, area increased the risk of exhibiting this frailty component in the youngest-old while decreasing the risk in the oldest-old.
Studies on contributing factors such as lifestyle habits, geographic location and type of work to the early manifestation of frailty remain scarce. The present study expands on previous work by exploring the relative contribution of these life-course factors to the manifestation of specific frailty components in the youngest-old. More specifically, the results showed that current smoking, but not past smoking, as well as lifetime number of cigarettes smoked were strongly related to the manifestation of one frailty component (low physical activity) earlier in life. Another important finding was the contribution of poor sleep to another frailty component (exhaustion), even though the relationship was not found exclusively in the youngest-old. Our study also confirmed moderate consumption of alcohol and, to a lesser extent, high consumption as a protective factor for three frailty components, and this relationship was found across all age groups. None of the life-course factors contributed significantly less to individual frailty components with advancing age, except for geographic location.
Our results are logically what one would expect, as smoking may increase the risk of being out of breath during physical activity, while poor sleep can lead to exhaustion. These findings are in agreement with recent studies [18,38], which identified current smoking but not past smoking as a predictor of frailty, compared to never smoking. Our results are also in line with Peterson [17], who did not find any relationship between smoking and a proxy measure of slowness (Short Physical Performance Battery), suggesting that smoking is related to some but not all frailty components. As for poor sleep, its association with frailty at all ages is consistent with conclusions from recent studies [15,17,39].
Our findings are also consistent with a recent review that concludes that moderate and high alcohol consumption may reduce the risk of frailty [38]. The protective effect of wine is also in agreement with the conclusions of earlier studies (e.g., Ortolá et al., 2016) [40], while the finding concerning drinking beer is more surprising. Our results did not concur with those obtained by Brunner [18], Peterson [17] and Strandberg [41], who found that frailty was associated with high alcohol consumption. The discrepancy with our results may be partly attributable to the way the variable measured was defined. “High” consumption (>1 drink per day) in our Canadian study may, in European studies, be referred to as “moderate” consumption [18,41], which has not been found to be related to frailty. Moreover, in the above studies, high alcohol consumption during midlife (50s), not current consumption later in life (65+), was associated with frailty, suggesting that lifelong drinking may have a different impact. These conclusions are also in agreement with our results showing that starting to drink later in life reduces the risk of exhibiting a frailty component (low physical activities) in the youngest-old only. However, memory bias due to cognitive decline cannot be excluded and might have masked a significant relationship between alcohol consumption and frailty by underestimating the percentage of heavy drinkers in the frailest participants.
Overall, we did not find an association between geographic location and frailty components in the youngest-old. These results are in line with a Canadian study [21], which found similar risks of frailty between rural and urban residents early in the aging process. Our unadjusted results, however, showed that living in an urban area increased the risk of exhibiting slowness at a younger age, when compared to a semi-rural area. Our findings can be interpreted in light of the specific urban area where the data were collected. Because Sherbrooke is one of the least wealthy cities in the province of Québec, the relationship between living area and frailty may be mediated by low income [42,43]; this was supported by the lack of a significant relationship found after controlling for socioeconomic variables (from p = 0.036 to p = 0.108, when education and income are added to gender and comorbidity). Interestingly, geographic location was found to be the only life-course risk factor where the contribution changes significantly with advancing age, indicating that living in an urban area decreased the risk of exhibiting slowness in the oldest-old, compared to those living in a semi-rural area. This finding may shed light on the mixed results found in past studies concerning the relationship between geographic location and frailty. Future studies may indicate which specific characteristics of these living areas, such as greater access to services income [44] or to neighborhood green spaces [45], might explain this shift throughout the aging process.
Concerning clinical implications, the present study highlights the potential relevance of: (1) helping the youngest-old to stop smoking and hopefully prevent or delay the early manifestation of frailty in this subgroup. Despite the challenges of giving up this habit in the context of lifelong dependence [46], the benefits of smoking cessation even at an older age (late 50 s/early 60 s) could be promoted through programs tailored to their specific needs; (2) investigating sleep quality when assessing frailty to potentially reduce exhaustion through appropriate interventions targeting physiological (apnea) or affective (depressive symptoms) factors. As the relationship between sleep disorders and exhaustion can be two-way [47,48], future studies should investigate whether poor sleep tends to be a cause of exhaustion in the youngest-old and a consequence of age-related fatigue in the oldest-old, which may suggest different treatments according to age; and (3) questioning whether the protective effect of moderate alcohol consumption, especially wine, is linked directly to alcohol, or whether it is a proxy measure of engagement in social activities [49]. This hypothesis is supported by recent data suggesting that social participation may reduce the risk of slowness in older adults [50], which is consistent with the significant relationship found in our study between this frailty component and moderate alcohol consumption.
Some limitations should be considered when interpreting our findings. First, a cross-sectional design was used, which precludes inferences regarding causal associations between contributing factors and frailty components. Second, the validity of self-reported data in our sample may have been affected by social desirability bias related to smoking and drinking or by subjective perceptions of poor sleep. Third, the selected variables for geographic location and type of work might have impacted the results since length of exposure, more than exposure per se, may mediate the relationship with frailty [51]. In this regard, a growing number of studies have warned that more attention should be paid to how outdoor and indoor air pollution toxicity may accelerate the frailty process [52–55]. Fourth, the impact of some potential confounding variables on the early manifestation of frailty, such as autism, intellectual disabilities [56] and HIV infection [57], were not specifically investigated, as they were not identified in the FRéLE database. These variables are, however, related to comorbidities, which were controlled for in our models. Finally, since the participants lived in a specific region of Canada, our findings may not be generalizable to other populations. On the other hand, the study used data from a large multicenter sample, stratified by living area (metropolitan, urban, semi-rural), which increases its external validity and applicability to community-dwelling older adults in general.
While other studies have sought to document the influence of physical, psychological and social factors in the manifestation of frailty, the contribution of lifestyle habits, geographic location and type of work to specific frailty components has received little attention. Moreover, to our knowledge, this is one of the few studies to specifically target the subgroup of youngest older adults. Our findings may support the adaptation of current public policy programs, such as those designed to help young older adults stop smoking, to prevent the early manifestation of frailty components. New tools promoting smoking cessation and monitoring sleep could sustainably complement public health strategies aimed at healthy aging for these specific risk factors. Prospective studies should shed more light on how the interaction of lifespan factors, such as toxicity exposure in the living environment and workplace, contributes to the early onset of frailty. Despite ethical and methodological challenges, other predictors, such as HIV infection and intellectual disabilities, should be included in future research.
VP, FB, JT designed the study. JT and VP conducted the literature review. CG, JF and FB performed the data collection. MPG, JF, FB, CG and JT analyzed the data. VP wrote the paper with input from all authors. All authors approved the final version to be published.
The authors declare that they have no conflicts of interest.
The FRELE study was supported by the Canadian Institutes of Health Research [grant numbers 82945]. The authors want to thank statistician Lise Trottier for her assistance with the statistical analyses. They also want to thank the study participants for taking parts in this project.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
Provencher V, Béland F, Galand C, Fletcher JD, Tuakuila J, Garant M-P. Contribution of Lifestyle Habits, Geographic Location and Type of Work to the Manifestation of Individual Frailty Components in the Youngest-Old. Adv Geriatr Med Res. 2020;2(4):e200021. https://doi.org/10.20900/agmr20200021

Copyright © 2020 Hapres Co., Ltd. Privacy Policy | Terms and Conditions




