Location: Home >> Detail
Adv Geriatr Med Res. 2020;2(4):e200025. https://doi.org/10.20900/agmr20200025

1 Faculty of Kinesiology and Recreation Management, University of Manitoba, Winnipeg, Manitoba R2H 2N2, Canada
2 Institute of Cardiovascular Sciences, St. Boniface Hospital Albrechtsen Research Centre, Winnipeg, Manitoba R2H 2A6, Canada
3 Max Rady College of Medicine, Rady Faculty of Health Sciences, University of Manitoba, Winnipeg, Manitoba R3E 0W2, Canada
4 Cardiac Sciences Program, Winnipeg Regional Health Authority, Winnipeg, Manitoba R2H 2A6, Canada
5 Department of Surgery, Max Rady College of Medicine, Rady Faculty of Health Sciences, University of Manitoba, Winnipeg, Manitoba R3E 0W2, Canada
* Correspondence: Todd A. Duhamel, Tel.: +1-204-235-3589.
This article belongs to the Virtual Special Issue "Frailty"
Background: Frailty and cardiovascular disease (CVD) share common pathophysiology in their progression. Declines in bone health often occur concomitantly with frailty and CVD. Therefore, analytes of bone metabolism may be useful biomarkers of pre-frailty and CVD risk. The aim of this study was to identify the effects of pre-frailty and CVD risk on the systemic concentrations of bone metabolism and inflammatory analytes in middle-aged and older females.
Method: This case-control study is a secondary analysis of data from 1030 females with no self-reported history of CVD. Frailty was measured using the Fried Criteria, and females were stratified into low and elevated CVD risk using the Framingham risk score. Greedy matching with pre-frailty as the exposure variable identified 26 matched pairs in the low and elevated CVD risk groups for a total of 104 females. Factorial ANOVA compared differences in the log transformed concentrations of 15 bone metabolism analytes based on pre-frailty status, CVD risk, and the interaction.
Results: Differences in the systemic concentrations of IL-6 (5.25 ± 14.30 vs 1.35 ± 1.74 pg/mL, p = 0.001), TNFα (1.41 ± 1.83 vs 0.89 ± 0.40 pg/mL, p = 0.06), and leptin (12628.48 ± 10472.90 vs 7562.96 ± 4972.25 pg/mL, p = 0.023) were found in elevated CVD risk status compared to low. No differences in the concentrations of bone metabolism analytes were found based on pre-frailty status, nor were any interaction effects.
Conclusion: Differences were found in the concentrations of cytokines involved in bone metabolism based on CVD risk; however, no differences were found based on pre-frailty status. IL-6, TNFα, and leptin may act as biomarkers of CVD risk, but this study does not support the use of the examined analytes involved in bone metabolism as biomarkers of pre-frailty.
CVD, cardiovascular disease; FRS, Framingham risk score; PHIN; Personal Health Identification Number; FC, Fried Criteria; HDL, high-density lipoprotein; ACTH; adrenocorticotropic hormone; DKK1, Dickkopf WNT signaling pathway inhibitor 1; IL-6, interleukin-6; TNFα, tumor necrosis factor α; OPG, osteoprotegrin; OC, osteocalcin; OPN, osteopontin; IL-1β, interleukin-1 β; PTH, parathyroid hormone; FGF23, fibroblast growth factor 23
The population of Canada is aging rapidly. Currently, 17% of the population is 65 and older [1], and this proportion is expected to reach 25% by 2036 [2]. From a public health perspective, this is likely to result in increasing prevalence of both frailty [3] and cardiovascular disease (CVD) [4] as the presence of these conditions is associated with age.
Frailty is characterized by a state of increased vulnerability to health stressors resulting from the dysregulation of multiple physiological systems [5]. This leads to a reduction in physiological reserve and an impaired ability to respond to adverse health events [6]. Pre-frailty is an intermediary stage preceding frailty that increases risk of frailty progression [6]. Individuals who are pre-frail are able to respond to health stressors [7], but are still at increased risk for disability, mortality, and morbidities, including CVD [6,8].
Frailty and CVD share similar risk factors and pathophysiological progression [9]. Sarcopenia and osteoporosis, as well as chronic inflammation [10] are often associated with both conditions. As a result, the presence of frailty and CVD are thought to exacerbate each other [11]. Recently, large pooled data sets have identified that frail individuals are at increased risk for CVD [12,13] and this increased risk is apparent in the earlier pre-frail stage [13–15]. This relationship is also bidirectional as individuals with a high CVD risk had an increased risk for incident frailty over a 4 year period (OR 2.15; 95% CI 1.68–2.75) [16].
Biomarkers of both frailty and CVD are beginning to be examined with the goal of accurately identifying at-risk individuals earlier in downward health trajectory [17,18]. For example, blood-based biomarkers of inflammation have been studied as biomarkers of frailty in the younger-old and the very-old [19]. Given the related pathophysiology of frailty and CVD [9,20], these conditions may share common biomarkers.
Bone and muscle are both highly dynamic organs which secrete cytokines that act throughout the body [21–24]. The cross-talk between bone and muscle is receiving increased attention as it may have a role in health maintenance and decline [24–25]. Dysregulation in bone-muscle cross-talk can influence the progression of osteoporosis and sarcopenia [26] conditions often seen in frailty [27,28]. Pre-frail and frail individuals are at increased risk for osteoporotic fracture [29,30] and have been shown to present with reduced bone health [31,32]. Bone and cardiovascular health are also suggested to be linked, since reduced bone health is associated with increased risk for CVD, and vice versa [33,34], potentially implicating this same dysregulated cross-talk in CVD progression. Specifically, females who are post-menopause may be at increased risk for frailty-related reductions in bone and cardiovascular health, as hormonal changes post-menopause increase risk for both osteoporosis and CVD [35,36]. Bone metabolism analytes have previously been measured in the systemic circulation as a means of assessing bone health [22,37]. Given the relevance of bone metabolism and bone-muscle cross-talk to frailty characteristics and cardiovascular health, it is possible that these analytes may act as biomarkers of frailty and CVD.
The objective of this study was to identify the main and interaction effects of pre-frailty and CVD risk on the systemic concentrations of bone metabolism and inflammatory analytes in middle-aged and older females. Reduced bone health can occur concomitantly with frailty and CVD; therefore, bone metabolism analytes may be useful biomarkers of pre-frailty and CVD risk. The identification of biomarkers in the early pre-frailty stage could allow for easier detection and tracking of frailty progression [28].
The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement guidelines for case-control studies were adhered to in the development of this manuscript [38]. This case-control study was a secondary analysis of data previously collected from an observational cohort study [39] approved by the University of Manitoba Health Research Ethics Board on September 29, 2014 (H2014:224) and the St-Boniface Hospital Research Review Committee on March 13, 2015 (RRC/2014/1417). The initial study examined the sensitivity and specificity of novel CVD risk assessment methods for predicting CVD events, such as the standardized Fried Criteria (FC) [40] and the Rasmussen Disease Score [41], as compared to established approaches, such as the Framingham Risk Score (FRS) [42].
ParticipantsThe initial observational cohort study was conducted in Winnipeg, Manitoba, Canada and recruited 1030 females using radio and media ads. Participants were included if they were a female aged 55 years or older with no previous self-reported CVD, had a Personal Health Information Number (PHIN), and if informed consent was obtained. Participants were excluded if they had been previously hospitalized for CVD, as described in the protocol paper [40]. Propensity matching with pre-frailty as the exposure variable was then used to identify a top set of 26 matched pairs in the low and elevated CVD risk groups for a total of 104 females to better control for potential confounding variables (Figure 1).
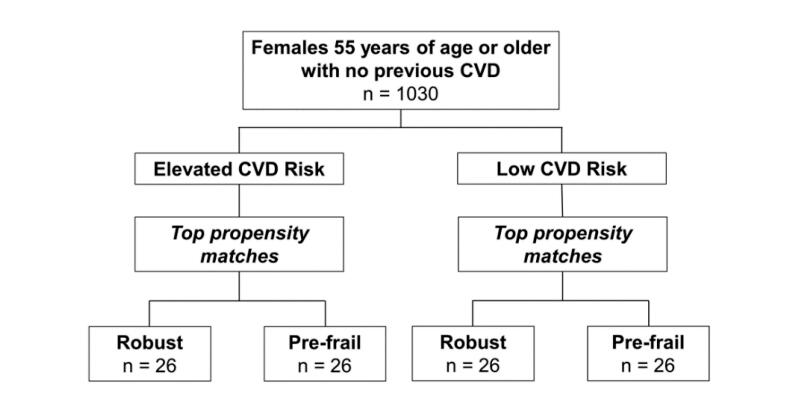 Figure 1. Study Flow Diagram.
Figure 1. Study Flow Diagram.
The FC was used to assess the frailty phenotype [6]. The FC assesses the presence of five criteria: (1) low physical activity levels; (2) slow walking speed; (3) muscle weakness (grip strength); (4) self-reported exhaustion; and (5) unintentional weight loss. Frailty status is determined using the number of criteria present (i.e., 0 = robust, 1-2 = pre-frail, ≥3 = frail). The cut-offs demarcating the presence or absence of the criteria were based on those of Fried et al [6].
Participants were instructed to fast for 12 h pre-appointment. Fasted blood samples were collected from all 1030 females. Immediately following sample collection, blood was centrifuged at 2000× g for 10 min at 4 °C. Plasma was then aliquoted into microcentrifuge tubes and stored at −80 °C for future analyses.
The FRS was determined based on the model of D’Agostino et al. [42]. High-density lipoprotein (HDL) and total cholesterol were measured using the collected plasma. Resting blood pressure was measured in a supine position, following 10 minutes of rest, in a calm environment at room temperature. Resting blood pressure was measured using the HD/PulseWaveTM CR-2000 Research CardioVascular Profiling System (Hypertension Diagnostics, Minneapolis, MN, USA). Participant sex, age, smoking status, diabetes status, and blood pressure treatment status were collected from participant questionnaires.
The systemic concentrations of bone metabolism analytes were measured with a EMD Millipore MILLIPLEX® Map Human Bone Magnetic Bead Panel—Bone Metabolism Multiplex Assay (EMD Millipore, Burlington, MA, USA) [43]. This multiplex assay allows for the concurrent quantification of adrenocorticotropic hormone (ACTH), Dickkopf WNT signaling pathway inhibitor 1 (DKK1), interleukin-6 (IL-6), insulin, tumor necrosis factor α (TNFα), leptin, osteoprotegrin (OPG), osteocalcin (OC), osteopontin (OPN), interleukin-1 β (IL-1β), parathyroid hormone (PTH), and fibroblast growth factor 23 (FGF23). These analytes were selected due to their roles in bone metabolism, amongst others. Plasma samples used in the analysis of the analytes were collected simultaneously as the plasma samples used in the FRS analysis.
Statistical AnalysisParticipants were classified as low CVD risk (FRS < 10%) or elevated CVD risk (FRS ≥ 10%). Propensity scores based on a greedy match were calculated for the low and elevated CVD risk participants with the exposure variable of pre-frailty status, creating a case-control design with four groups: (1) Low FRS-Robust; (2) Elevated FRS-Robust; (3) Low FRS-Pre-frail, and; (4) Elevated FRS-Pre-frail. Propensity scores matched females for age, body mass index, continuous FRS, smoking status, and the number of currently prescribed medications. The analyte concentrations were log transformed to adjust for skewness and reduce variability in the data set. Factorial ANOVA compared the main and interaction effects of pre-frailty and CVD risk on the log-transformed systemic plasma concentration of 12 bone metabolism analytes. A Tukey post-hoc test was used to compare means where significant difference (p-value ≤ 0.05) was found. The study was powered using the concentration of the inflammatory cytokine IL-6 from a similarly aged cohort [44] (distribution of 9.5 ± 2.5 pg/mL (Mean ± SD)), a total sample size of 80 (20 in each group) was calculated to detect a 25% difference between groups (80% power; two-tailed alpha = 0.05). All statistical calculations were made using SPSS version 26 (IBM Corporation, Armonk, NY, USA).
Characteristics of the low and elevated CVD risk propensity matched groups were similar (Table 1). Mean age was lower in the robust group as compared to the pre-frail group in females of low CVD risk (62.92 ± 4.89 vs 65.58 ± 7.10 years, p = 0.02). Differences were found in the prevalence of post-secondary education (22 (84.6%) vs 15 (57.7%), p = 0.03), HDL cholesterol (1.63 ± 0.43 vs 1.88 ± 0.61 mmol, p = 0.04) and small artery compliance (3.80 ± 2.44 vs 2.62 ± 1.13 mL/mmHg×10, p = 0.01) between females who were robust and females who were pre-frail in the elevated CVD risk group. All females were post-menopause.
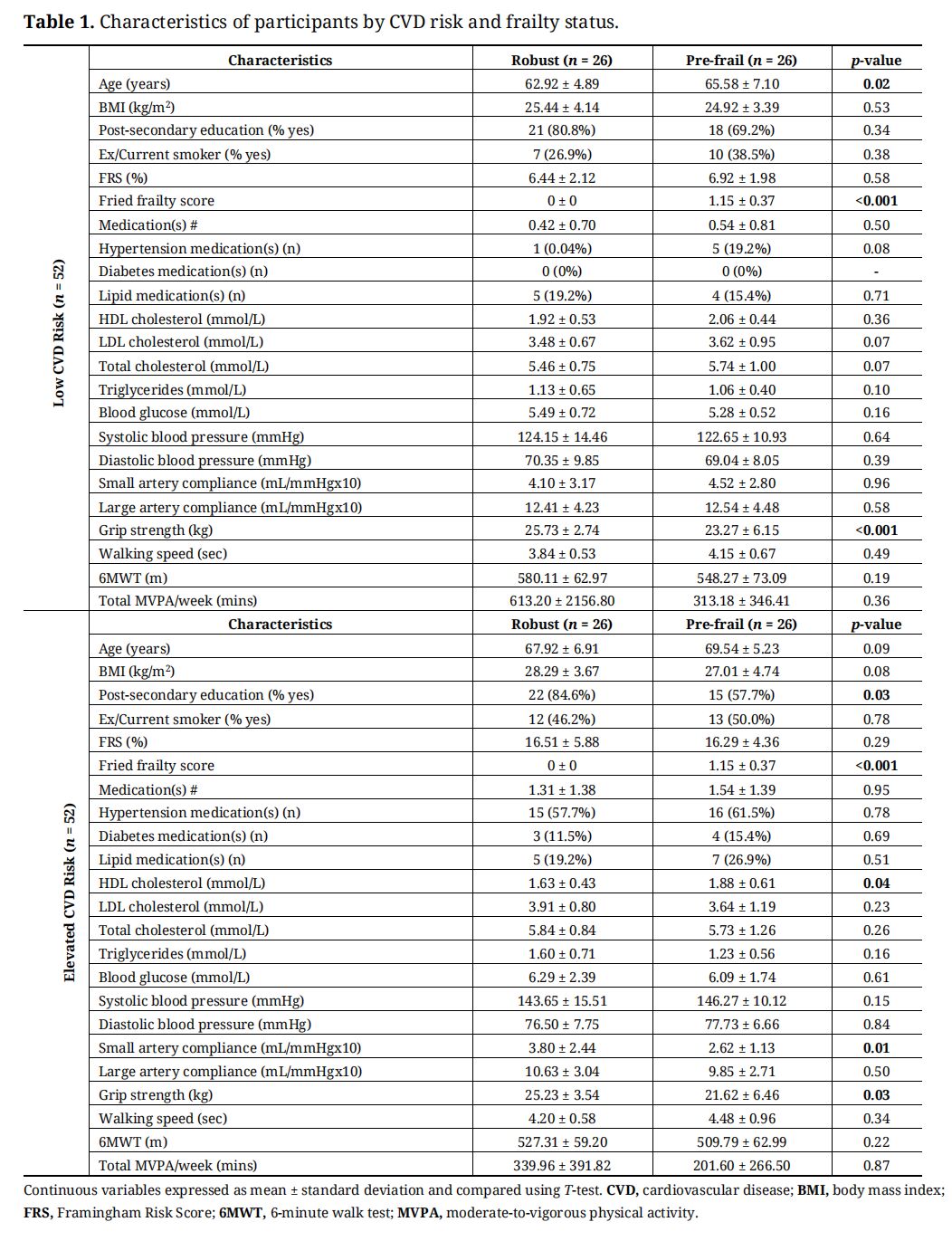 Table 1. Characteristics of participants by CVD risk and frailty status.
Table 1. Characteristics of participants by CVD risk and frailty status.
The main effects for pre-frailty and CVD risk status and their interaction effects are found in Table 2. ACTH and PTH were not included in the final analysis as concentrations in the majority of the samples measured below detectable limits for the assay. Significantly higher concentrations were present in females of elevated CVD risk, as compared to those of low CVD risk for IL-6 (5.25 ± 14.30 vs 1.35 ± 1.74 pg/mL, p = 0.001), TNFα (1.41± 1.83 vs 0.89 ± 0.40 pg/mL, p = 0.006), and leptin (12628.48 ± 10472.90 vs 7562.96 ± 4972.25 pg/mL, p = 0.023). No differences in the concentrations of bone metabolism analytes were found based on pre-frailty status. No interaction effects between pre-frailty status and CVD risk were found.
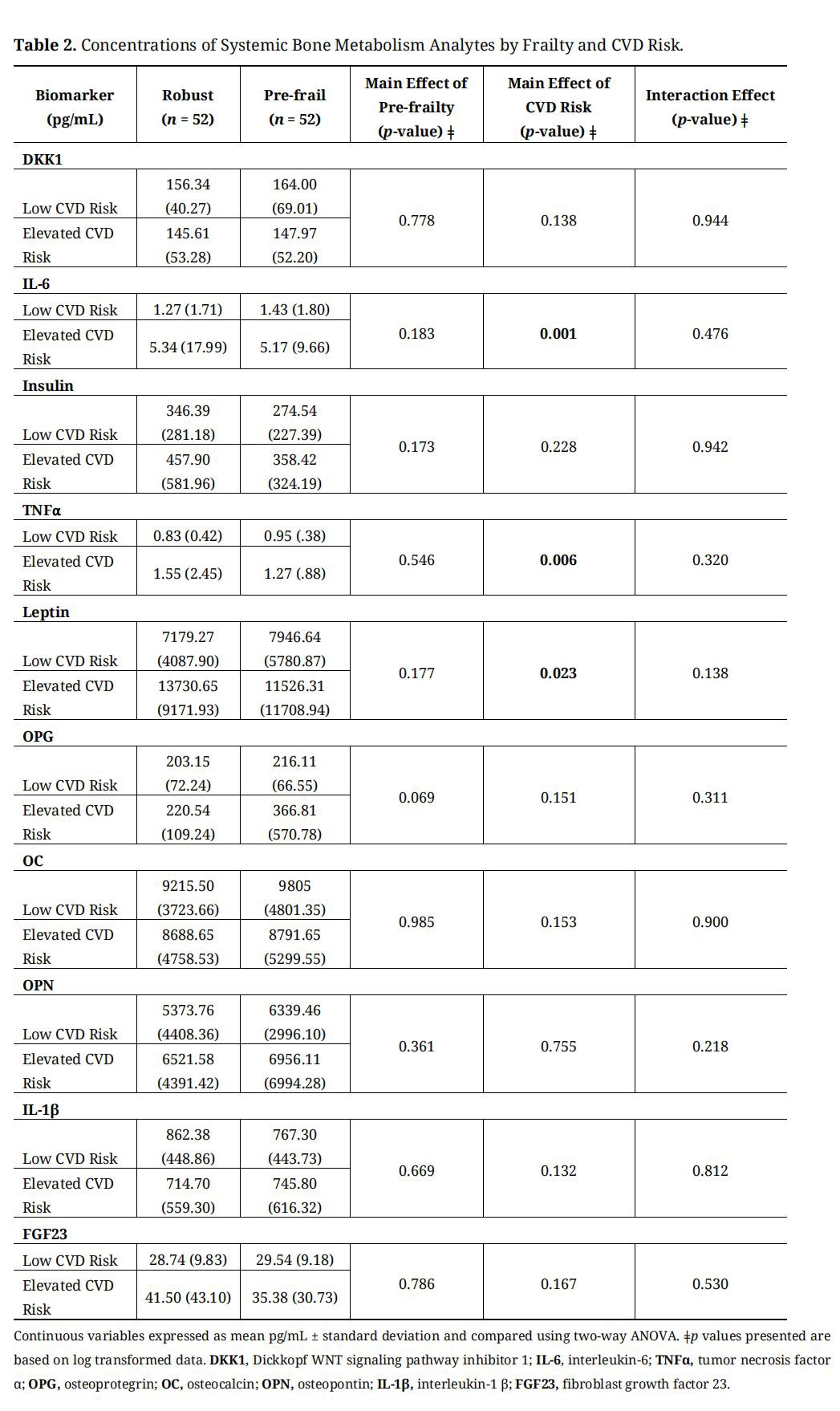 Table 2. Concentrations of Systemic Bone Metabolism Analytes by Frailty and CVD Risk.
Table 2. Concentrations of Systemic Bone Metabolism Analytes by Frailty and CVD Risk.
No differences in the concentrations of the assessed bone metabolism analytes were found in females who were pre-frail, compared to those who were robust, and no interaction effects were found between pre-frailty and CVD risk status. Based on these findings, analytes involved in bone metabolism may not be useful biomarkers of pre-frailty.
Reductions in bone health may occur concomitantly with frailty [32] as frailty has been predictive of osteoporotic fractures [45]. There is some evidence to suggest changes to bone health in the earlier, pre-frail stage as reduced bone mineral density has been identified in pre-frail females [46], but this research was on a slightly older cohort (mean age = 70 years). Pre-frail males have been found to have reduced bone health compared to frail males, as assessed by quantitative ultrasound [33]. Though, the bone mineral density scans of these pre-frail males were not significantly different from the robust group, indicating only early changes to bone health [32]. We found no differences in the concentrations of bone metabolism analytes between pre-frail and robust females. This may be because pre-frailty is too early in frailty progression for changes in bone health to be detected with biomarkers associated with bone metabolism. As such, differences in the concentrations of bone metabolism analytes between these two groups may not be identifiable until later frailty stages. Markers of bone metabolism have been reported to be higher in females with established frailty [47]. Therefore, had this study utilized females who were frail instead of pre-frail and who were older, differences in the concentrations of bone metabolism analytes between groups might have been found. This finding could warrant the use of alternative biomarkers allowing for early identification and intervention prior to the onset of associated adverse health outcomes. Thus far, evidence suggests that interventions implemented in the earlier pre-frail stage are more likely to successfully slow or reverse frailty progression [48].
Although no differences were found in the concentrations of bone metabolism analytes based on pre-frailty, differences were found based on CVD risk status. IL-6, TNFα, and leptin were higher in females at elevated CVD risk, as compared to females at low CVD risk.
IL-6 is an inflammatory cytokine typically involved in the body’s immune response [49]. IL-6 has a wide range of inflammatory effects throughout the body [50] and it is involved in bone metabolism [51]. IL-6 has been reported to stimulate the genesis of osteoclasts, multinucleated giant cells with the capacity to breakdown bone tissue [52]. Thus, increased inflammation is associated with reduced bone mass [53]. Increased inflammation is also implicated in the development of CVD [54] and frailty [55]. We identified higher levels of IL-6 in females at elevated CVD risk, however, there was no difference in IL-6 concentration between robust and pre-frail females. Despite this finding, increases in IL-6 have often been identified in pre-frail and frail individuals [56]. This discrepancy may have resulted from the large variations in IL-6 concentrations between groups which might have impacted our ability to identify higher levels of IL-6 in pre-frail females. In relation to CVD, the higher levels of IL-6 found in females at elevated CVD risk status is supported by previous evidence identifying IL-6 as a biomarker of CVD [57].
TNFα is also an inflammatory cytokine with an important role in the immune response and has pleiotropic effects throughout the body [58]. Like IL-6, TNFα is able to induce osteoclastogenesis, leading to the destruction of bone tissue [59]. Additionally, TNFα is able to suppress the activity of osteoblasts, cells responsible for forming new bone [60], further reducing bone health. As such, this inflammatory cytokine is thought to be associated with altered bone metabolism [61]. TNFα has already been identified as a biomarker of CVD [62] and because of its link with inflammation, evidence also supports its use as a potential biomarker of frailty with higher levels often being present in pre-frail and frail individuals [56]. Higher levels of TNFα were identified in females at elevated CVD risk but frailty status did not influence TNFα concentration in our study participants. Again, this discrepancy may be due to large variations in the concentration of this cytokine between groups. Past research supports the finding of higher levels of TNFα found in individuals at elevated CVD risk [63], indicating the efficacy of this cytokine in CVD risk assessment.
Leptin is a hormone predominately synthesized and secreted by adipocytes [64]. Leptin regulates bodyweight and energy balance [65], yet also has a complex role in bone metabolism [66,67]. The specific effects of leptin on bone metabolism are difficult to summarize [68], though research suggests leptin is necessary for both the inhibition and stimulation of bone formation [69,70]. A relationship between leptin and CVD has been established [71] and the use of leptin as a biomarker of CVD is supported by clinical studies demonstrating increased concentration of leptin is predictive of cardiovascular events [72]. Additionally, leptin concentrations are higher in obesity and other metabolic disorders which predispose for the development of CVD [73]. Thus, the increase in leptin concentration present in females at elevated risk for CVD might result from the presence of metabolic risk factors for CVD in this group.
LimitationsDespite using results from a similarly aged cohort to calculate sample size for this study [44], large variations in the concentrations of bone metabolism analytes in the systemic concentration were found within groups. This variation may have impacted our ability to identify differences between groups. The specific cause of this variation is unclear, and improved methodological approaches are needed to address variability in the future [74]. The measured analytes, while selected for their involvement in bone metabolism, also play a variety of pleiotropic roles throughout the body, such as the well-known roles of IL-6 and TNFα in inflammation [49,58]. This makes conclusively stating which pathophysiological processes connect the studied analytes to outcomes like pre-frailty or elevated CVD risk difficult to ascertain. Further, the collection of bone mineral density measures and information on potential hormone replacement therapies in the females of this cohort could have provided additional information on the bone health of the participants, which may have assisted in explaining why the bone metabolism analytes were not found to be effective biomarkers of pre-frailty.
Future DirectionsThere is an increasing need to identify and validate biomarkers of pre-frailty and frailty as current identification is based on specific criteria which can sometimes be inconsistent [75]. While the measurement of bone metabolism analytes is effective in the monitoring of conditions like osteoporosis [76], bone metabolism analytes may not be useful biomarkers of pre-frailty as reductions in bone health may only be evident later in the frailty progression of most females. Additional research is necessary to (1) identify biomarkers of pre-frailty; (2) define the physiological ranges of these biomarkers; (3) identify the optimal method of assessing established biomarkers; and (4) examine the underlying pathophysiology connecting said biomarkers to frailty progression in more detail.
These findings will support the development of novel biomarker-based methods of pre-frailty and CVD risk assessment. The identification of effective biomarkers of pre-frailty may be used to identify potential physiological dysfunction, facilitate early intervention, and lead to the development of therapeutic strategies [77]. Promising biomarkers of pre-frailty and CVD may be identified in our cohort in 2022, following the completion of a 5-year follow up period [39].
No differences were found for the concentrations of any bone metabolism analytes based on pre-frailty status, nor were any interaction effects between pre-frailty and CVD risk. It is possible these females were too early in the progression of frailty to have developed reductions in bone health that were detectable using biomarkers of bone metabolism. Concentrations of IL-6, TNFα, and leptin were found to be higher in females who were at elevated risk of developing CVD, as compared to females at low risk for developing CVD. This research suggests these cytokines involved in bone metabolism may act as potential biomarkers of CVD risk; however, it did not identify potential biomarkers of pre-frailty in middle-aged and older females.
TAD and KFB were involved in conception and design of the research. TAD and KFB obtained ethics approval. KFB, CJO, LAT, and TAD drafted the manuscript. All authors edited and revised the manuscript. All authors approved the final version of the manuscript. CJO performed data analysis. BMH provided statistical support.
The authors declare no conflicting interests.
This study was financially supported by an operating grant from the St. Boniface Hospital Foundation, Winnipeg, Manitoba, Canada. KFB is supported by a Frederick Banting and Charles Best Canada Graduate Scholarship–CIHR Doctoral Award. CJO is supported by a Frederick Banting and Charles Best Canada Graduate Scholarship–CIHR Master’s Award.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
68.
69.
70.
71.
72.
73.
74.
75.
76.
77.
Boreskie KF, Oldfield CJ, Thompson LA, Moffatt TL, Hiebert BM, Arora RC. Bone Metabolism Analytes as Biomarkers of Pre-Frailty and Cardiovascular Disease Risk in Females. Adv Geriatr Med Res. 2020;2(4):e200025. https://doi.org/10.20900/agmr20200025

Copyright © 2020 Hapres Co., Ltd. Privacy Policy | Terms and Conditions




