Location: Home >> Detail
Adv Geriatr Med Res. 2025;7(2):e250007. https://doi.org/10.20900/agmr20250007
 ,
Irene Cho 2
,
Irene Cho 2
1 S R Nathan School of Human Development, Singapore University of Social Sciences, Singapore 599494, Singapore
2 Department of Economics and Cognitive Science, University of Chicago, Chicago, IL 60637, United States
* Correspondence: Cheng Kian Kelvin Tan.
According to the World Health Organisation (WHO), there are nearly 20 million new cancer cases in 2022. In a rapidly ageing world, coupled with improved lifespan, the total number of cancer diagnoses is likely to increase. Cancer patients face significant stress and fatigue from managing the condition and treatment. In mitigating these challenges, the care sector is embarking on use of non-pharmacolgical therapeutic interventions. Virtual Reality technology and music are feasible tools for improving mental wellbeing, relaxation and pain reduction. The systematic review was conducted across five databases between June 2024 and July 2024. Twelve shortlisted studies were examined, which used nature-based, interactive and non-interactive, and meditative VR interventions, VR interventions combined with physiotherapy, background music, or drugs; and standalone music interventions. The studies were conducted in various cancer populations, including advanced cancer patients, end-stage cancer patients in hospice care, breast cancer patients with chronic pain, cancer survivors with chronic cancer-related pain, and metastatic breast cancer patients. Most studies used a range of pre- and post-intervention measurements of anxiety, depression, pain, and other symptoms, and some included control groups or control conditions. The review provides a comprehensive synthesis of research on VR and music as psychosocial interventions for adult cancer patients. mixed results for the effects of these interventions on anxiety, depression, pain, fatigue, sleep, and other psychophysical outcomes. Overall, VR and music may be the basis of promising interventions for cancer patients, but further research is needed.
IARC, international agency for research on cancer; World Health Organization, WHO; HADS, hospital anxiety and depression scale; SAI, state anxiety inventory; DASS, depression, anxiety, and stress scale; GAD, general anxiety disorder test; CNSVS, CNS vital signs; AVLT, auditory verbal learning test; TMT-A, Trail-Making Test-A; TMT-B, Trail-Making Test-B; PCI, perceived cognitive impairment; ACA, perceived cognitive ability; VFT, verbal fluency test; BPI, brief pain inventory; VAS, visual analog scale; CSQ, coping strategies questionnaire; ESAS, edmonton symptom assessment system; EQ-5D-5L, EuroQol-5 Dimensions-5 Levels; FACIT-Fatigue, functional assessment of chronic illness therapy—fatigue scale; INS, inclusion of nature in the self; ISI, insomnia severity index; SAS, self-rating anxiety scale; SDS, self-rating depression scale; PSQI, Pittsburgh sleep quality index; WHOQOL-BREF, World Health Organization quality of life brief version
According to the latest estimates from the World Health Organisation (WHO), there were nearly 20 million new cancer cases and 9.7 million cancer deaths in 2022. Lung cancer was the most common cancer globally, with 2.5 million new cases, accounting for 12.4% of the total. Female breast cancer ranked second, with 2.3 million cases (11.6%), followed by colorectal cancer with 1.9 million cases (9.6%). The estimates also indicate that approximately 1 in 5 people will develop cancer during their lifetime [1].
The IARC predicts that over 35 million new cancer cases will occur in 2050, representing a 77% increase from 2022. This rapidly growing global cancer burden is attributed to increased exposure to risk factors, such as air pollution, and to major changes in population demographics [2]. Specifically, by 2050, the number of individuals aged 60 years and older is expected to double globally, from 1 billion in 2020 to 2.1 billion, and the number of individuals aged 80 years or older is projected to triple during this period, reaching 426 million [3].
Age is the most important risk factor for cancer overall and for many individual cancer types. Cancer incidence rates steadily increase with age, rising from fewer than 25 cases per 100,000 people in those under 20 to about 350 per 100,000 among individuals aged 45–49, and exceeding 1,000 per 100,000 in those aged 60 and older [4]. By 2030, 70% of all cancer diagnoses are expected to occur in adults aged 65 and older. Consequently, although age-specific cancer mortality is decreasing due to improved prevention, the total number of cancer diagnoses and death rates continues to rise, with population ageing being the primary cause [5].
In adopting a multidimensional problem solving approach, studies will provide insight into the psychosocial wellbeing of participants [6]. Cancer patients face significant stress due to physically demanding treatments and the resulting permanent health impairments, disabilities, fatigue, and pain that persist even after the cancer has been treated [7]. Fatigue is the most commonly reported symptom of cancer and cancer treatments and is often cited as causing the greatest interference with daily activities. Estimates of fatigue rates among cancer patients vary widely, ranging from 4% in breast cancer patients before chemotherapy to 91% in those who have undergone surgery and chemotherapy and are awaiting bone marrow transplantation. Additionally, an estimated one third to one half of patients undergoing cancer treatment experience pain that can persist even when no signs of cancer remain [8]. The fatigue, pain, and other physical ailments experienced by cancer patients and survivors often hinder their ability to perform routine activities of daily living, including bathing, using the toilet, dressing, preparing meals, and feeding themselves. The impact on daily living can contribute to emotional distress and mental health issues among cancer patients, potentially leading to significant social problems, such as an inability to work and reduced income [7].
In addition to these physical stressors, the emotional stress of living with a cancer diagnosis and the fear of recurrence can exacerbate or introduce new psychological distress [7]. A study conducted at a U.S. cancer centre, which included nearly 4500 patients aged 19 and older, found that significant psychological distress was reported by 29% to 43% of those with the 14 most common types of cancer [9]. Moreover, even patients who do not exhibit these clinical syndromes may still experience substantial psychological stress, such as worries, fears, guilt, loss of control, anger, sadness, and confusion [10]. Common psychological issues among these patients include anxiety, mood disturbances, fear of recurrence, concerns about body image, and difficulties in communication with family members [7].
Virtual Reality and Music as Non-Pharmacological Therapeutic InterventionsNon-pharmacological interventions are defined as science-based and non-invasive interventions that aim to prevent, treat, or cure health problems. They have a measurable impact on health, quality of life, and behavioural markers and are associated with biological and/or psychological processes identified in clinical studies. Among the types of non-pharmacological interventions are psychological interventions, such as stress management and relaxation techniques (i.e., meditation, mindfulness practices) and cognitive-behavioural interventions (i.e., problem-solving, cognitive restructuring, role-playing) [11].
One emerging field of research is the use of virtual reality (VR) technology in non-pharmacological health care applications. As developments in mobile phones and head-mounted displays make virtual reality (VR) more accessible, it is rapidly becoming an appealing tool for the health care industry [12]. VR consists of a three-dimensional, computer-generated environment viewed through a head-mounted display and a tracker that updates the image based on the users’ movements. This allows images to change naturally with head motion, providing a sense of immersion. Numerous studies have demonstrated the efficacy of VR interventions in managing psychosocial symptoms, with the majority focusing on VR-based exposure therapies for the treatment of mental disorders and phobias [13,14], VR experiences for pain reduction [15,16], and VR relaxation experiences for people with mental health conditions [17–19].
Scientific research has shown that music can influence physiological processes that enhance physical and mental well-being. Music therapy is defined as the clinical and evidence-informed use of music interventions to accomplish individualised goals within a therapeutic relationship [20]. Studies on patients diagnosed with mental disorders such as anxiety, depression, and schizophrenia have identified visible improvement in patients’ mental health after general music and music therapy interventions [20–23].
Given these insights, there is a compelling rationale to integrate VR and music therapy into psychosocial treatments for cancer patients and survivors as non-pharmacological interventions for any disorders or distress they may experience. In this paper, we review studies that have examined the use of VR and music interventions for adult cancer patients (who are not undergoing cancer treatments like chemotherapy during the intervention) and cancer survivors. We focus on how these interventions impact outcomes related to psychosocial well-being, such as anxiety, depression, cognitive function, pain, fatigue, and sleep. The review presents findings on the systems used as interventions, the psychological and psychophysical effects associated with these interventions, and the limitations of these studies.
The review was conducted across five databases, namely PubMed, Web of Science, Scopus, Elsevier, and ProQuest, between June 2024 and July 2024. The following keywords were used: ((cancer) AND (elderly)) AND (community) AND (music) OR (virtual reality) AND ((anxiety) OR (depression)) AND NOT ((education) OR (performance) OR (pediatric) OR (cardiac) OR (dental) OR (oral) OR (pregnant) OR (surgical) OR (perioperative) OR (balance) OR (autism) OR (schizophrenia) OR (classroom) OR (covid)). Keywords were used to search titles, abstracts, and the full text of the articles that had the keywords in the titles or abstracts.
Inclusion and Exclusion CriteriaWe included articles that (1) involved VR and/or music interventions for cancer patients and/or survivors; (2) provided qualitative and/or quantitative outcome measures; due to the limited number of studies. Our exclusion criteria were (1) review papers, books, or book chapters; (2) studies published before July 2014; (3) studies involving paediatric participants; (4) studies that administered the VR and/or music intervention during cancer treatment (e.g. during chemotherapy); (5) studies published in languages other than English’; and (6) studies that used technological interventions other than VR, such as augmented reality.
Screening and Data ExtractionTitles and abstracts identified in the initial search were screened to exclude unrelated articles. The full-text screening was performed in two steps. First, the text of each article was searched for the keywords and studies that did not include any of the keywords were dropped from the sample. Second the inclusion/exclusion criteria were applied to the remaining papers. We then collected detailed information from each article in the final sample. Specifically, we extracted the following data: study information (first author, year of publication), demographics (number of subjects, gender distribution, age), study design (control group, exclusion criteria, target population, target problem, experiment description, stimulated sense), intervention (VR/music device), and outcomes (psychological measurement indicators, results extracted from physiological measurements, follow-up findings).
Our initial keyword search identified 6109 articles: 800 from PubMed, 3325 from ProQuest, 1984 from Web of Science, and none from Elsevier or Scopus. After the complete screening process, the sample consisted of 12 articles (summarised in Tables 1 and 2) examining the effects of VR and/or music interventions on various psychosocial outcomes for cancer patients. The studies examined the use of VR and/or music therapy in various cancer populations, including advanced cancer patients, end-stage cancer patients in hospice care, breast cancer patients with chronic pain, cancer survivors with chronic cancer-related pain, and metastatic breast cancer patients. The studies used a range of pre- and post-intervention measurements of anxiety, depression, pain, and other symptoms, and some included control groups or control conditions.
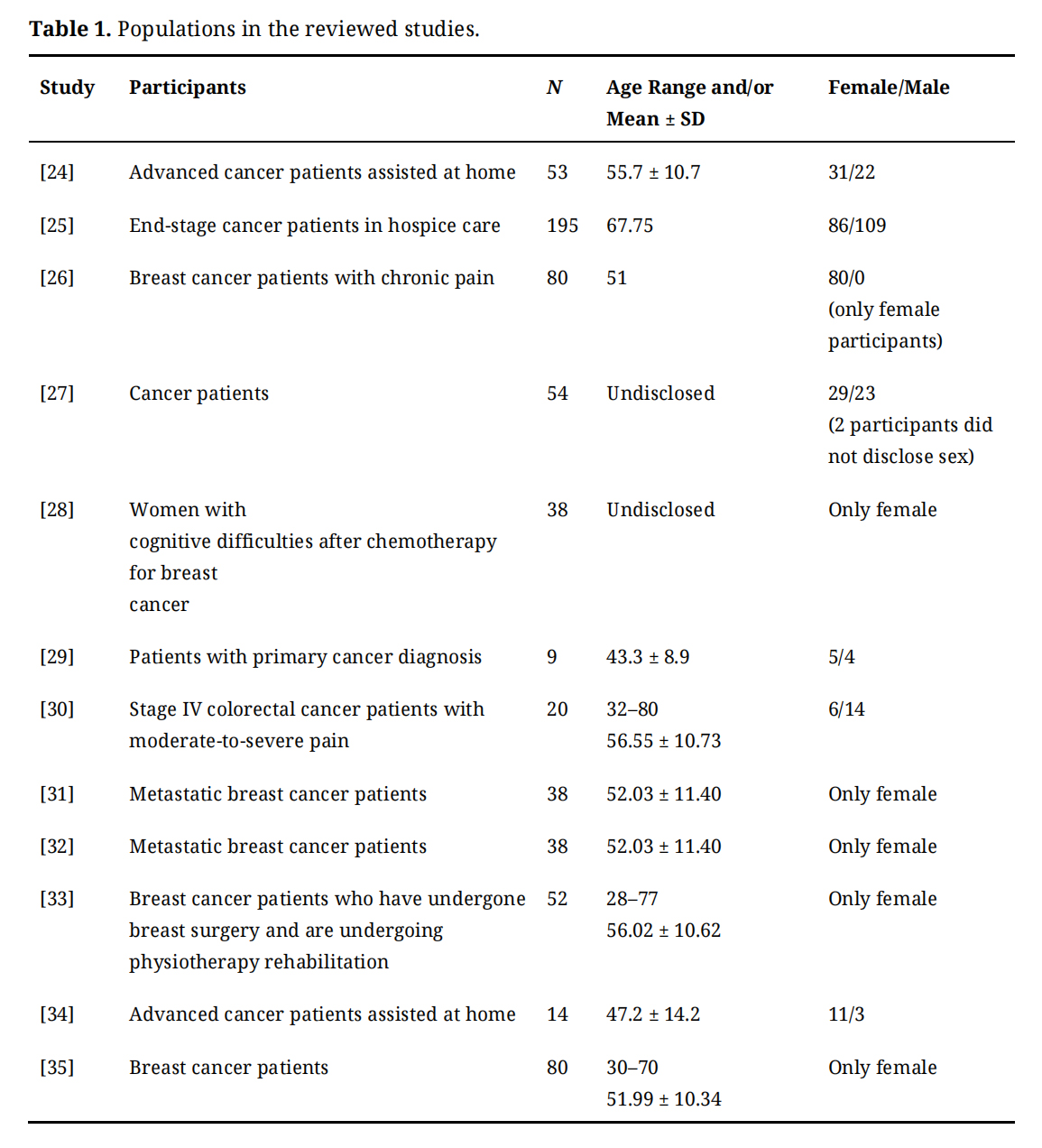 Table 1. Populations in the reviewed studies.
Table 1. Populations in the reviewed studies.
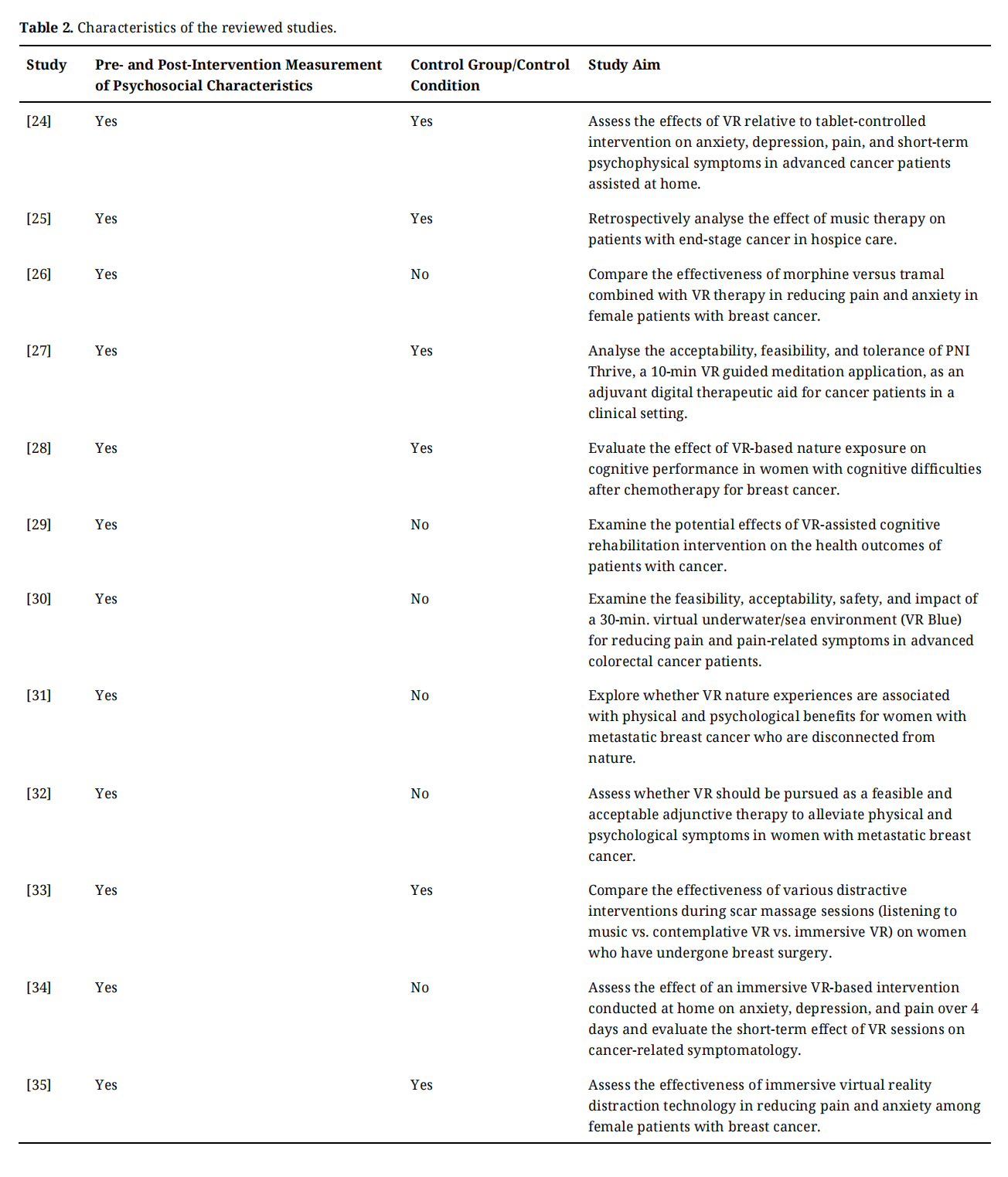 Table 2. Characteristics of the reviewed studies.
Table 2. Characteristics of the reviewed studies.
In Table 3, eleven studies [24,26–35] examined the effects of a VR intervention. With the exception of two studies [28,29] that did not specify the VR environment shown to participants, all of the studies used VR environments consisting of relaxing experiences of nature, such as underwater scenes, outdoor camping, beaches, waterfalls, and mountain ranges. One study [27] featured an outer space environment and also included scenes of the destruction of cancerous cells and, for religious participants, the Star of Bethlehem.
Music interventionWhile several studies incorporated music into their interventions, only two studies [25,33] specifically examined the effects of music on patients. Dong and Qu [25] analysed the effect of music therapy on patients with end-stage cancer in hospice care, using lively, melodious, and relaxing tunes chosen according to the patients’ personal music preferences for daily listening. In contrast, Buche et al. [33] compared the effectiveness of listening to music, specifically Vivaldi’s ‘Spring’ from The Four Seasons, with a VR intervention during a physiotherapy session for breast cancer patients.
VR and music combined interventionFour studies [27,30–32] combined VR and music in their interventions. Although none of these studies specifically aimed to evaluate the effects of music, they incorporated soothing/relaxing background music into the VR interventions.
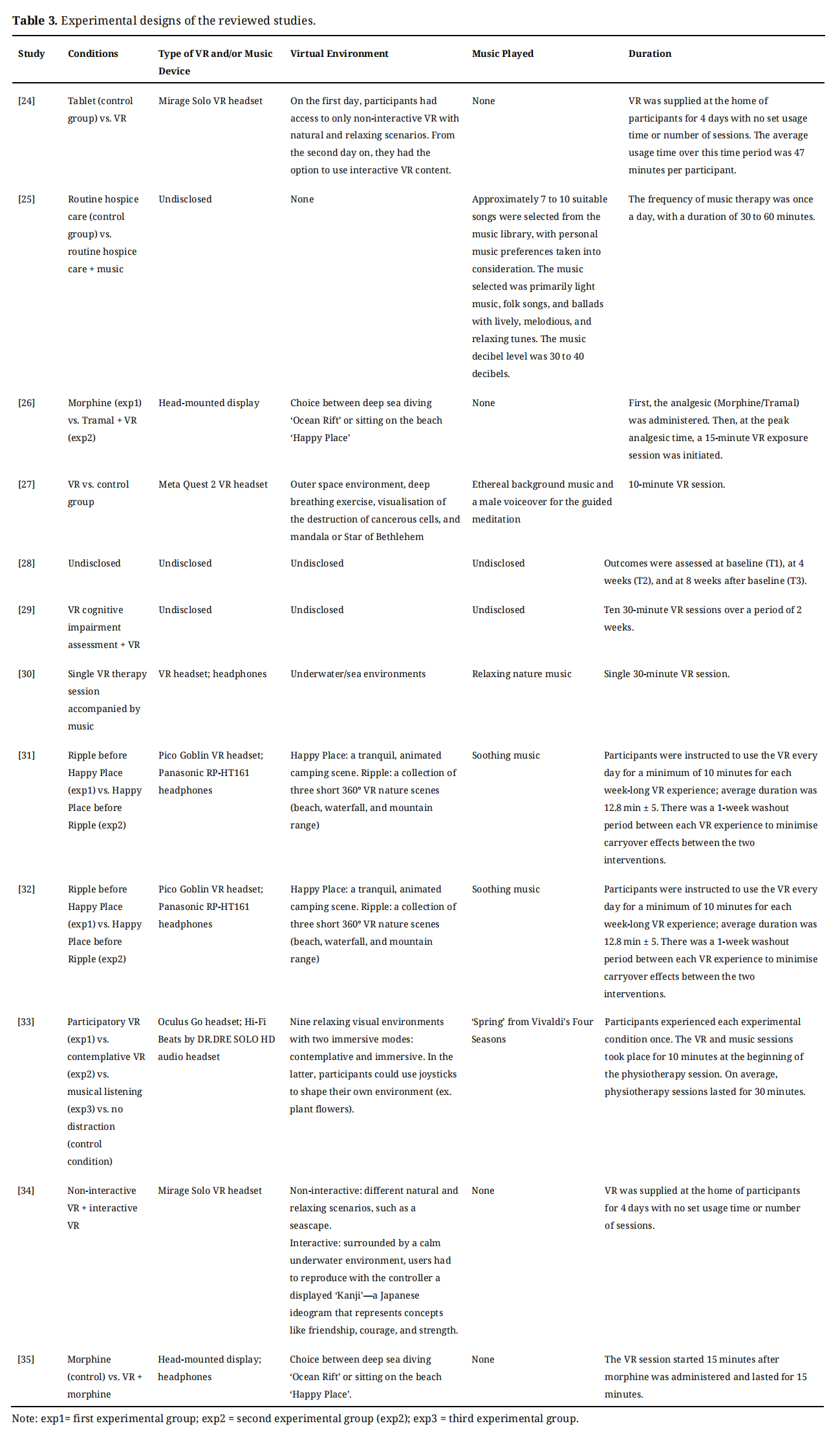 Table 3. Experimental designs of the reviewed studies.
Table 3. Experimental designs of the reviewed studies.
Eight studies (summarised in Table 4) evaluated the effect of VR on reducing anxiety [24,26,31–35]. Two studies used the Hospital Anxiety and Depression Scale (HADS) [24,34], three studies used the State Anxiety Inventory (SAI) [26,33,35], two studies used the Depression, Anxiety, and Stress Scale Short Form (DASS-SF) [31,32], and one study used the General Anxiety Disorder Test (GAD) [29]. All of the described assessments were subjective, self-reported measures. Of the eight studies, five reported a statistically significant reduction in anxiety among participants receiving the VR intervention [24,31–33,35]. Reynolds et al. [32], using a sample of metastatic breast cancer patients, compared baseline measurements with measurement taken at the end of the week-long VR experience and in a follow-up measurement 48 hours after the end of the experience. Anxiety decreased between the pre- and post-intervention measurements but was only significantly lower than at baseline in the follow-up measurement. The studies that did not report statistical significance were Zeng et al. [29], Moscato et al. [34], and Ahmad et al. [26]. Ahmad et al. [26] compared the effects of VR combined with Tramal, a weak opioid, with those of morphine, a strong opioid, alone. They found no significant difference between the two experimental groups, and both groups experienced a significant reduction in anxiety. Thus, combining VR with weak opioids like Tramal was demonstrated to be nearly as effective as using strong opioids like morphine for reducing anxiety in breast cancer patients.
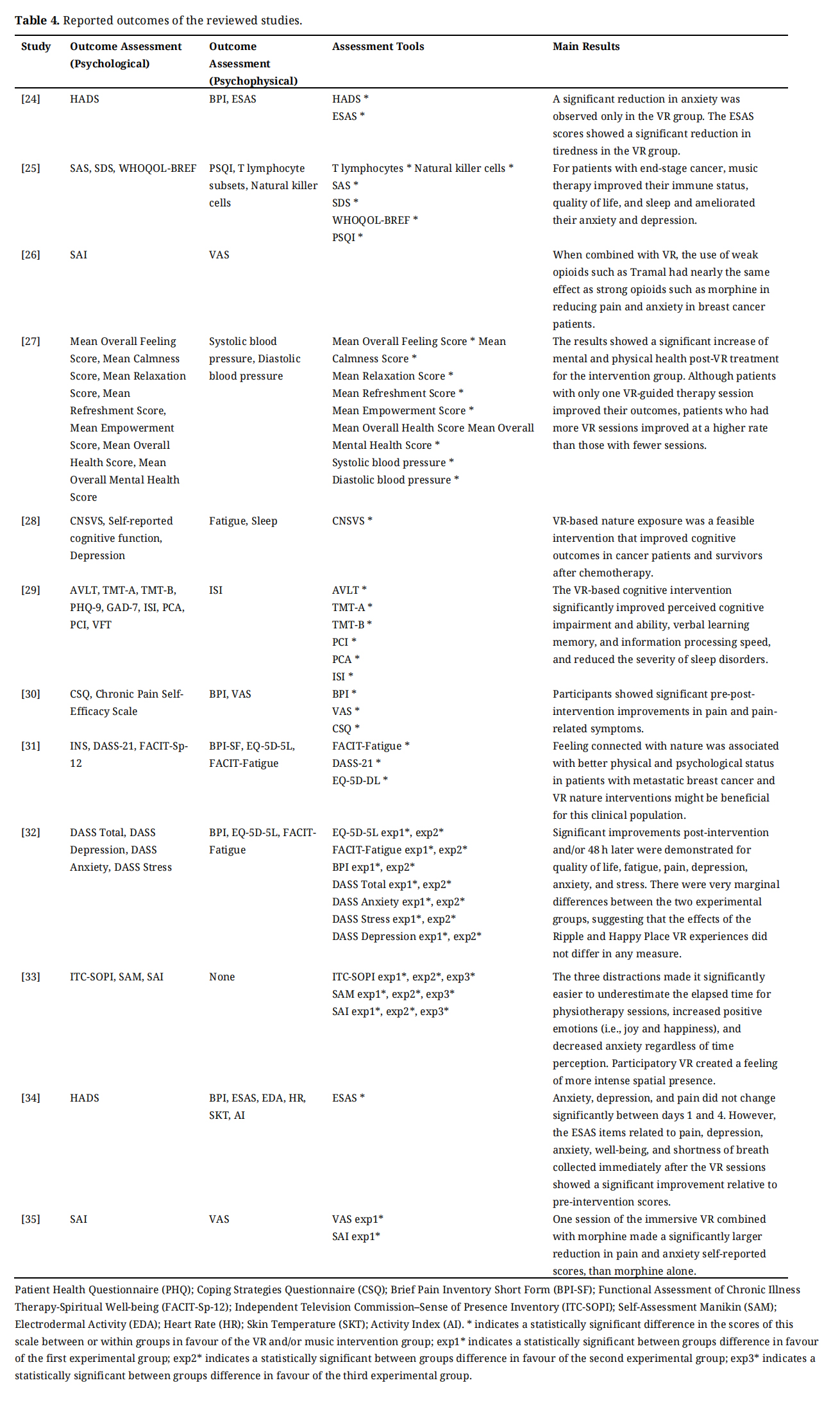 Table 4. Reported outcomes of the reviewed studies.
Table 4. Reported outcomes of the reviewed studies.
Six studies evaluated the effect of VR on alleviating depression [24,28,29,31,32,34]. Two studies reported statistically significant reductions in depression [31,32]. Chin et al. [31] explored whether VR nature experiences were associated with physical and psychological benefits for women with metastatic breast cancer who were disconnected from nature. Using the DASS, they found that those with a weaker baseline connection with nature showed significant improvements in depression following the intervention, providing evidence that VR nature interventions are beneficial for this clinical population. Reynolds et al. [32] also used the DASS to measure changes in depression and found a significant decrease in depression between the pre- and post-intervention periods. However, the follow-up conducted 48 hours later did not show further statistically significant improvement. Giannelli et al. [24], Jung et al. [28], Zeng et al. [29], and Moscato et al. [34] found no significant reductions in depression levels after the interventions.
Cognitive functionTwo studies examined the effects of VR on cognitive impairment and ability. Jung et al. [28] used self-reported assessments of cognitive function and CNS Vital Signs (CNSVS); the participants were women with cognitive difficulties following chemotherapy for breast cancer. CNSVS is a computerised neurocognitive test battery developed as a routine clinical screening instrument. It consists of seven tests: a test of verbal and visual memory, finger tapping, symbol digit coding, the Stroop Test, a test of shifting attention, and the continuous performance test. The participants showed significant improvement in CNSVS scores, indicating that VR-based nature exposure is a feasible intervention that can enhance cognitive outcomes in cancer patients and survivors after chemotherapy. Zeng et al. [29] used the Auditory Verbal Learning Test (AVLT), Trail-Making Test-A (TMT-A), Trail-Making Test-B (TMT-B), Perceived Cognitive Impairment (PCI), Perceived Cognitive Ability (ACA), and Verbal Fluency Test (VFT). They found significant improvements in all measures except for the VFT, indicating that VR-based cognitive interventions significantly improved perceived cognitive impairment and ability, verbal learning memory, and information processing speed.
Other psychological outcomesFranklin et al. [27] used pre- and post-treatment surveys of their own design to assess psychological outcomes. Each patient was asked to evaluate and report their feelings about their condition, their health, and their outlook by responding to a survey questionnaire. The questionnaire used items rated on a scale of 0 to 6 to collect data on seven psychological/mental wellness-related areas: Overall Feeling, Calmness, Relaxation, Refreshment, Empowerment, Overall Health, and Overall Mental Health. Statistically significant improvements were recorded for the means of all seven categories post-VR treatment in the intervention group. Furthermore, although patients with only one VR-guided therapy session showed improved outcomes, those who had more VR sessions improved at a higher rate than those with fewer sessions.
Outcome Assessment of the VR Intervention (Psychophysical) PainSeven studies examined the effects of VR interventions on pain intensity [24,26,30–32,34,35]. Three of these studies reported significant reductions in pain [30,32,35]. Kelleher et al. [30] investigated pain and pain-related symptoms in advanced colorectal cancer patients, finding that the pain experienced ‘right now’ decreased by 58.93% between the pre- and post-VR measurements, based on the results of the BPI. Additionally, tension decreased by 74.33%, as measured by the Visual Analog Scale (VAS). The study also assessed changes in cognitive variables related to pain, including pain catastrophising (the tendency to make negative self-statements and catastrophise when faced with pain) and pain self-efficacy (the confidence in one’s ability to reduce pain and continue daily activities). A significant correlation was found between changes in pain catastrophising, as determined by the Coping Strategies Questionnaire (CSQ), and changes in relaxation. In Reynolds et al. [32], patients who received VR interventions had lower BPI scores post-intervention, but these reductions only reached statistical significance in the follow-up measurements. Mohammed and Ahmad [35] found that one session of immersive VR combined with morphine led to a significant reduction in pain, as measured by the VAS, compared with morphine alone in breast cancer patients. In contrast, no statistically significant reductions in pain were observed in Giannelli et al. [24], Chin et al. [31], or Moscato et al. [34], which used the BPI as the outcome measure, or in Ahmad et al. [26], which used the VAS. It is noteworthy that, similar to their findings for anxiety, Ahmad et al. [26] found no significant difference in pain reduction between morphine alone and Tramal combined with VR. However, both groups experienced a significant reduction in pain. Thus, combining VR with weaker opioids like Tramal was shown to be nearly as effective as using stronger opioids like morphine for reducing pain in breast cancer patients.
Multidimensional outcomesSeveral studies used multidimensional assessment tools to evaluate the multiple symptoms experienced by cancer patients. Giannelli et al. [24] and Moscato et al. [34] used the Edmonton Symptom Assessment System (ESAS), a comprehensive self-report tool for assessing the severity of nine common cancer symptoms: pain, tiredness, nausea, depression, anxiety, drowsiness, appetite, well-being, and shortness of breath. Giannelli et al.’s [24] analysis of the ESAS data showed a significant improvement in tiredness for the VR group. Moscato et al. [34] reported significant improvements in pain, depression, anxiety, well-being, and shortness of breath immediately after using VR. Additionally, an analysis of the correlations between the usage time of a single VR session and pre-post differences in ESAS scores revealed significant negative correlations for anxiety, worst feeling of well-being, and shortness of breath. It is noteworthy that the ESAS items related to anxiety, depression, and pain showed significant improvement, even though these symptoms did not show significant improvement when measured by the HADS or BPI in the same study. Chin et al. [31] and Reynolds et al. [32] used the EuroQol-5 Dimensions-5 Levels (EQ-5D-5L), a self-report assessment of mobility, self-care, usual activities, pain/discomfort, and anxiety/depression, to measure quality of life. Chin et al. [31] reported a significantly greater quality of life following the VR nature intervention compared with the baseline. Reynolds et al. [32] found a small but statistically significant increase in quality of life between the pre- and post-intervention periods.
Fatigue and sleepThree studies examined the effects of VR intervention on fatigue [28,31,32]. Two of these studies reported statistically significant improvements in fatigue, both using the Functional Assessment of Chronic Illness Therapy—Fatigue Scale (FACIT-Fatigue), a self-reported assessment of fatigue and its impact on daily activities and function [31,32]. In Chin et al. [31], there was a main effect of time on fatigue, with post-intervention fatigue being significantly lower than baseline fatigue. However, the interaction between time and connection with nature indicated a trend, with post hoc tests revealing that fatigue levels only improved in women with a weaker connection to nature (measured by Inclusion of Nature in the Self (INS) scores at baseline). In Reynolds et al. [32], fatigue significantly decreased between the pre- and post-intervention timepoints, and this improvement was maintained at a follow-up 48 hours later. Jung et al. [28] did not report significant improvements and did not disclose the outcome measure used to assess pre- and post-intervention changes in fatigue.
Two studies examined the effects of VR intervention on sleep [28,29]. Zeng et al. [29] used the Insomnia Severity Index (ISI) to assess the severity of sleep disorders in cancer patients, finding that the VR psychological intervention significantly reduced the severity of sleep disorders. Jung et al. [28], which did not disclose the outcome measure for sleep, did not find any significant improvements in sleep quality.
Other psychophysical outcomesTwo studies examined the effects of VR on a broad range of physiological outcomes [27,34]. Franklin et al. [27] measured patients’ blood pressure before and after the VR-guided meditation intervention, observing a statistically significant decrease in both systolic and diastolic blood pressure in the intervention group relative to the control group. A decrease in systolic blood pressure in particular has meaningful medical benefits. The authors argued that this result is evidence of the calming effect of the intervention. However, they also noted that other factors may influence blood pressure outcomes (such as rest, relaxation, posture) and that the effect of a patient’s current medication on blood pressure cannot be excluded. Based on the participants’ medication histories, there was a list of medications with potential effects on blood pressure.
Moscato et al. [34] used a smart wearable wristband to evaluate the effects of the VR intervention on four physiological signals: electrodermal activity (EDA), heart rate (HR), skin temperature (SKT), and activity index (AI). These physiological parameters were chosen because they have been extensively used in emotion recognition research, specifically in association with stress, pain, and the evaluation of depressive and anxious symptoms. The study found no significant changes in these signals before, during, or after the VR sessions. Although not statistically significant, the EDA progressively decreased over the three phases, while HR, SKT, and AI were lower during the VR sessions than in the 10-minute time windows before and after the intervention.
Outcome Assessment of the Music Intervention (Psychological and Psychophysical)Two studies examined the effects of music intervention on various outcomes in cancer patients [25,33]. Dong and Qu [25] assigned end-stage cancer patients in hospice care to either the conventional group (receiving routine hospice care) or the combination group (receiving both hospice care and music therapy). Before the study, there were no significant differences between the two groups in terms of immune indicators, anxiety and depression scores, quality of life scores, or sleep quality scores. After the intervention, patients in the combination group showed statistically significant improvements in all of the outcomes compared with the conventional group: higher immune status (as indicated by immune indicators lymphocytes CD3+ and CD4+), lower anxiety and depression scores (Self-Rating Anxiety Scale (SAS) and Self-Rating Depression Scale (SDS)), improved sleep quality scores (Pittsburgh Sleep Quality Index (PSQI)), and higher World Health Organization Quality of Life Brief Version (WHOQOL-BREF) scores in all domains. Additionally, the degree of decline in the physical, psychological, and social relationship domain scores was smaller in the combination group than in the conventional group.
There participants in Buche et al. [33] were women with breast cancer who had undergone breast surgery. These women participated in four experimental conditions during scar massage sessions, one of which included listening to music. The study measured the interventions’ effects on mood states and anxiety. It found an increase in positive emotional state and a decrease in negative emotional arousal after each session, as indicated by the Self-Assessment Manikin (SAM). Additionally, there was a statistically significant decrease in anxiety based on the SAI assessment.
Three studies (summarised in Table 5) assessed patient accessibility and satisfaction. Kelleher et al. [30] used a 10-item Client Satisfaction Questionnaire and post-VR interviews, which revealed the high acceptability of the VR intervention, with participants finding the headset easy and comfortable to use, and expressing a desire to engage with VR frequently, especially during times of high pain or anxiety. Reynolds et al. [32] assessed the likelihood of participants using VR again, reporting a mean score of 73.01 for its Happy Place simulation environment and 66.67 for the Ripple simulation environment, alongside qualitative feedback indicating that the participants found relaxation and nature to be enjoyable aspects of VR. Buche et al. [33] collected written feedback, noting strong support for VR use post-immersion, with few participants experiencing discomfort and many reporting a feeling of losing track of time during the sessions.
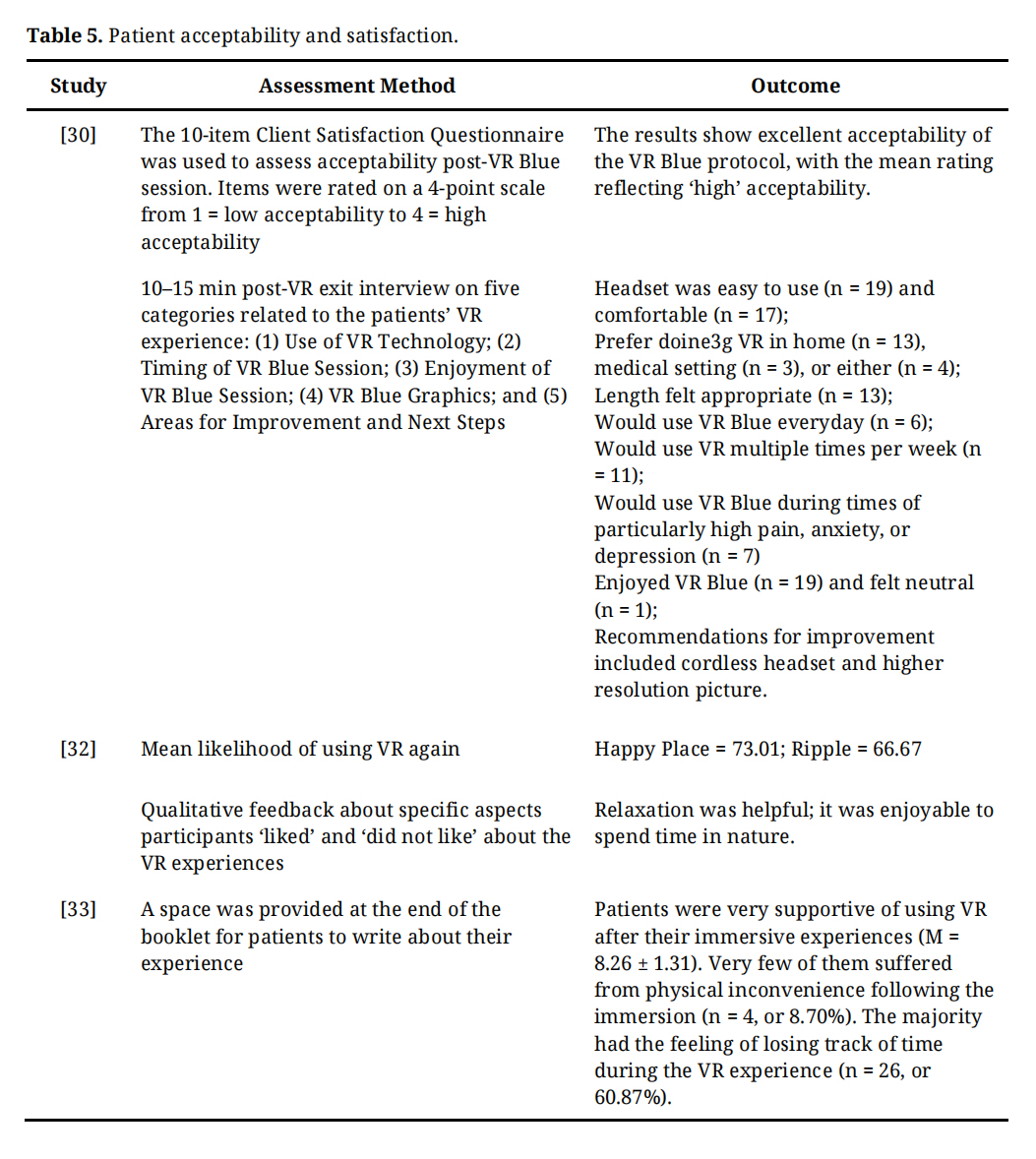 Table 5. Patient acceptability and satisfaction.
Table 5. Patient acceptability and satisfaction.
The reliability of the reported findings in several studies was compromised by small sample sizes; for example, in Zeng et al. [29], n = 9 and in Moscato et al. [34] n = 14. In Zeng et al. [29], the small sample size was due to a dropout rate of 50%, which may have also introduced attrition bias. Small sample sizes can result in poor statistical power, making it challenging to detect true effects or differences, and may lead to results that are not replicable. Researchers should aim to increase sample sizes in future studies. Larger sample sizes would improve the statistical power and robustness of the findings, contributing to more reliable and valid research outcomes.
Furthermore, 6 of the 12 studies focused solely on breast cancer patients [26,28,31–33,35], and one study examined only colorectal cancer patients [30]. While these studies provide useful results for these specific cancer diagnoses, they are not generalisable to all cancer patients, especially the breast cancer studies, which exclusively examined female participants. Future studies could consider including larger and diverse patient groups to benefit more cancer patients.
Another major limitation was the lack of studies on cancer survivors who have already undergone treatments such as chemotherapy. Only two studies examined this population [28,33]. Future research should focus on this group, as targeted studies can provide important insights into psychosocial therapies for cancer survivors, about 25% of whom experience persistent problems, including anxiety, depression, and other psychological and psychosocial distress [36].
Lack of control group/variablesSeven of the studies lacked a control group, assessing only a single group at baseline and post-intervention [26,29–34]. It should be noted that Buche et al. [33] had a single group of participants undergo four experimental conditions, one of which was a control condition. The absence of a proper control group makes it uncertain whether the outcomes were caused by the intervention or other variables. Having a control group strengthens the validity of a study’s conclusions and reduces the likelihood of erroneous interpretations.
In addition, several studies did no control some of the variables in their interventions, for example, by providing patients with VR systems in their homes without restrictions on usage time or number of sessions [24,29,31,32,34]. This introduces uncontrollable variables, such as patients’ usage patterns and the context in which they used the VR. These factors may have affected the outcomes in various ways; for example, some participants might have used the intervention for durations that were too short to yield significant improvements or in noisy environments that disrupted the intervention.
Furthermore, several studies that investigated the effects of VR included ‘soothing’, ‘relaxing’, or ‘ethereal’ background music during the intervention [27,30–32]. Accordingly, improvements attributed to the VR treatment may have been influenced by the music. There is a lack of studies specifically examining the independent effects of music interventions, further focused investigations in this area can yield new finding.
Study duration and lack of follow-upSeveral studies had short study periods or administered the intervention only once to participants. Giannelli et al. [24] and Moscato et al. [34] evaluated the effects of VR over 4 days, Ahmad et al. [26] and Mohammed and Ahmad [35] each offered a single 15-minute VR session, Franklin et al. [27] administered a single 10-minute VR session, and Buche et al. [33] conducted one 10-minute intervention session for each experimental condition (VR and music included). More studies should be conducted over a longer period with multiple intervention sessions and checkpoints for measuring outcomes. This would allow researchers to assess the effects and changes over an extended timeframe.
None of the studies, with the exceptions of Chin et al. (2022) [31] and Reynolds et al. [32], included follow-up testing. It should be noted that Chin et al. [31] was a secondary analysis of data collected by Reynolds et al. [32], so the data collection methodology was the same for both studies. The results of Reynolds et al. [32] highlighted the importance of conducting follow-up assessments: BPI, DASS Total, DASS Anxiety, and DASS Stress scores all improved and became significant only at a follow-up measurement conducted 48 hours after the intervention. This suggests that the full effects of the interventions may not be immediately apparent. Therefore, future studies should include follow-up assessments.
Lack of objective measuresIn addition to assessing cognitive function and physiological indicators such as blood pressure and immune status, all of the studies used subjective measures such as self-assessments, scales, and indexes to evaluate psychosocial outcomes including anxiety, depression, pain, quality of life, sleep, feelings, calmness, relaxation, refreshment, and empowerment. These subjective measures have limitations, including variations in individual interpretation, difficulty in quantifying experiences, inconsistencies in reporting, and susceptibility to biases such as social desirability.
Future research would benefit from complementing questionnaires with objective measures such as EDA, which provides real-time data on sympathetic nervous system activity that increases during physiological and emotional arousal. EDA was used in one of the studies reviewed [34].
Lack of studies examining the effects of a music interventionWhile several studies incorporated music into their VR interventions, only two studies [25,33] specifically examined the effects of music on patients. As a result, there is no clear consensus or comprehensive understanding of the effects of music therapy on various psychosocial outcomes for cancer patients.
Recommendations for future researchFuture studies in this field should address several key limitations identified in this review to enhance the robustness and applicability of their findings. First and foremost, there is a clear need to increase sample sizes. Many studies, such as those by Zeng et al. [29] and Moscato et al. [34], suffered from small sample sizes that undermined the statistical power and generalisability of their results. Increasing the number of participants will improve the reliability of results and enable researchers to detect true effects more accurately. Additionally, studies should aim for a more diverse participant pool beyond specific cancer types or treatment stages. Many studies focused exclusively on breast cancer patients or failed to include cancer survivors who had completed treatments like chemotherapy. Expanding research to a broader range of cancer diagnoses and stages will provide critical insights into the needs of different patient populations.
Another important area for improvement is the inclusion of control groups and the management of intervention variables. Several studies lacked proper control groups, making it difficult to attribute observed outcomes solely to the intervention rather than to external factors. Furthermore, the uncontrolled variables, such as patients’ usage patterns of VR and the presence of background music, may have confounded the results. Future studies should include well-defined control groups and standardise intervention conditions to accurately isolate the effects of the VR treatment.
In addition, as commented upon by Buche et al. [33], it could be helpful to offer a familiarisation step for the use of VR before starting the actual intervention. This preliminary phase would reduce the surprise effect and the naive attractiveness of VR, leading to a more accurate measurement of the emotional states associated with its use. Studies that have implemented a familiarisation phase in their research protocol have all observed significant results in reducing anger, pain, anxiety, or symptom distress [33]. Therefore, we can assume that there is a link between familiarisation and the significant results obtained from immersive experiences.
The duration and follow-up periods of the interventions also warrant attention. Many studies used short intervention periods or single-session protocols, which may not capture the full impact of the treatment. Additionally, the absence of follow-up assessments in most studies limits the understanding of the interventions’ long-term effects. Future research should extend the duration of interventions and incorporate follow-up evaluations to assess the sustainability of the outcomes and provide a more comprehensive view of the interventions’ impact over time.
Lastly, integrating objective measures into the assessments to complement the subjective assessments will enhance the reliability of the psychosocial outcome evaluations. While subjective measures are valuable, they are prone to biases and variability in interpretation. Incorporating objective indicators, such as EDA, can provide more reliable data on physiological and emotional responses and provide an understanding of the mechanisms through which the interventions affect these responses. Additionally, more research is needed to understand the specific impact of music interventions on psychosocial outcomes. Although some studies have included music as a component of VR interventions, there is limited research on its standalone effects, highlighting the need for focused studies in this area.
Addressing these recommendations will contribute to more rigorous, generalisable, and comprehensive research, ultimately enhancing our understanding of effective psychosocial interventions for cancer patients.
This systematic review provides a comprehensive synthesis of research on VR and music as psychosocial interventions for adult cancer patients. Twelve studies were examined, which used nature-based, interactive and non-interactive, and meditative VR interventions; VR interventions combined with physiotherapy, background music, or drugs; and standalone music interventions. The studies reported mixed results for the effects of these interventions on anxiety, depression, pain, fatigue, sleep, and other psychophysical outcomes. The review also provides a discussion of several limitations of these studies and recommendations for future studies. In future studies, objective physiological measures (e.g., biomarkers, electrodermal activity) can be incorporated alongside traditional assessments to validate findings more robustly. Adopting longer-duration interventions and incorporate regular follow-up evaluations will better assess long-term efficacy and sustained effects.
Overall, VR and music may be the basis of promising interventions for cancer patients, but further research is needed.
Not applicable.
Both authors discussed the results and contributed to the final manuscript.
No data were generated from the study.
The authors declare that they have no conflicts of interest.
We appreciate the support of the SUSS (Singapore University of Social Sciences)-Nunchi Marine Age Well Programme.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
Kelvin Tan CK, Cho I. Effects of Virtual Reality and Music Therapy on the Psychosocial Outcomes of Adult Cancer Patients: A Systematic Review. Adv Geriatr Med Res. 2025;7(2):e250007. https://doi.org/10.20900/agmr20250007

Copyright © Hapres Co., Ltd. Privacy Policy | Terms and Conditions




