Location: Home >> Detail
Adv Geriatr Med Res. 2025;7(3):e250013. https://doi.org/10.20900/agmr20250013

Department of Psychiatry, Azienda USL Toscana Nord Ovest, Lucca 55100, Italy
* Correspondence: Leonardo Massoni
Background: Parkinson Disease (PD) as well as other parkinsonisms such as Lewy Body Dementia (DLB), are often associated with neuropsychiatric symptoms. Hallucinations, apathy, dysphoria, anxiety, and aberrant motor behaviors are common neuropsychiatric features of both PD and DLB. The overlapping between Alzheimer disease (AD), PD, and DLB seems to be genetic, biological, clinical, and pharmacological.
Methods: In this review, a literature search was carried out to analyze the correlation between genetic, molecular, neurophysiological aspects, and neuropsychiatric symptoms of the above-mentioned diseases.
Results: Apolipoprotein E-4 (APOE-4), serotonin transporter gene (SLC6A4), and single nucleotide polymorphisms (SNPs) of glucocerebrosidase (GBA) are some of the main altered genes in AD, PDD and DLB. From a molecular point of view, α-synuclein and β/τ-amyloid are the main-altered proteins whose alteration has been implicated in neuropsychiatric symptoms of the diseases, while the entorhinal and parahippocampal regions, medial temporal lobes, limbic regions, and brain stem are the main impaired cerebral regions. Electrophysiological studies provided some insights into the prevalence of neuropsychiatric alterations, including visual hallucinations and poorer cognitive performance, especially in DLB, and pointed out an hypometabolism in frontal, parietal, and temporal lobes in AD.
Conclusions: Overall, AD, PD, and DLB may share clinical, neurochemical, and morphological characteristics, thus leading some authors to conceive a Lewy body disease spectrum. Further studies are warranted to find out clinical and neuropathological elements helping differential diagnosis between AD, PD dementia (PDD) and DLB.
Dementia is a progressive cognitive decline, accompanied by language and memory impairment as well as by mood and behavior alterations, finally leading to social and occupational problems with a significant impact on daily life activities [1,2]. DLB, PD, and AD are part of the degenerative diseases' spectrum and are associated with different levels of psychiatric and cognitive impairment. Dementia arising in a patient with a previous PD diagnosis is commonly defined PDD.
PD and DLB are known as α-synuclein (α-syn) pathologies, while AD is classically associated with amyloid β (Aβ) accumulations [3]. α-syn and Aβ are amyloidogenic proteins that tend to accumulate as insoluble fibrillary deposits in the brain of patients suffering from neurodegenerative diseases, including AD, PD, and DLB [4]. Wakasugi & Hanakawa (2021) proposed that the reciprocal relationship between α-syn and amyloid accumulation, as well as prion-like progression, may explain the overlapping pathology between AD and DLB [5]. The two pathologies also share anatomical aspects, such as the thinning of the entorhinal cortex [6]. In this framework, neuroimaging studies, including positron emission tomography (PET), are sometimes useful to detect similar or different functional aspects between the two diseases [7].
From a clinical point of view, Kaur and colleagues questioned if extrapyramidal signs (EPS) could be advantageous for differential diagnoses between AD and DLB. In fact, DLB patients generally exhibit a higher level of EPS, including Masked Facies, Rigidity, Resting Tremor, Impaired Posture/Gait, Speech/Hypophonia, Bradykinesia and Action/Postural Tremor if compared to AD individuals [8]. However, AD, PD, and DLB share neuropsychiatric symptoms such as delusions, hallucinations, and apathy [9].
In terms of therapeutic strategies, cholinesterase inhibitors, antidepressants, anxiolytics and antipsychotics are the most prescribed drugs for neuropsychiatric symptoms of the disease [10].
This review, starting from a general description of clinical aspects, analyses the genetic, molecular, biological, and electrophysiological mechanisms underlying the above-mentioned diseases, and gives some insights into the respective therapeutic implications.
To find out the main existing literature regarding genetic, molecular, biological, electrophysiological, and neuropsychiatric features of AD, PD, and DLB, a literature search was carried out by means of the “PubMed” database. Keywords employed were “neuropsychiatric symptoms”, “Alzheimer Disease”, “Parkinson Disease”, “Lewy Body Dementia”, “therapy”, “overlap”, “diagnostic”, “clinical”. Exclusion criteria were: (1) studies dealing with other than neuropsychiatric aspects of AD, PD, and DLB; (2) studies not carried out in human models; and (3) works not written in English. The literature review was conducted till February 2025. After an initial search, a total of 281 studies were identified. Articles not matching the above-mentioned characteristics were removed (n = 37) and the remaining 244 were considered for inclusion. Among them, 85 were assessed as eligible for inclusion and 71 of them were finally included in the “Results” section of the manuscript (see Figure 1).
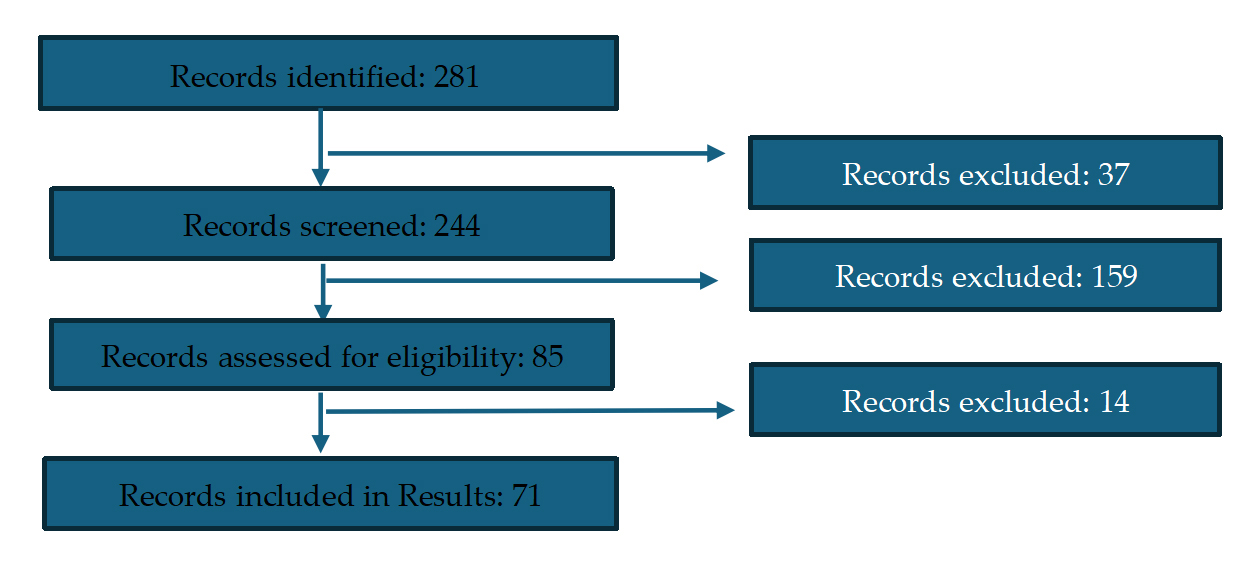 Figure 1. PRISMA flowchart of the literature search strategy.
Figure 1. PRISMA flowchart of the literature search strategy.
According to current diagnostic criteria, differential diagnosis between PDD and DLB is based on temporal sequence of symptoms appearance. Specifically, guidelines stress the timing of dementia. In fact, when dementia appears before parkinsonism, the diagnosis should be DLB, while when cognitive impairment follows motor symptoms, we should opt for PDD [9,10]. It should also be considered that DLB is often characterized by psychiatric symptoms, including suicide thoughts, even though not generally associated with a specific plan or desire of death [11]. About sleep, DLB individuals tend to have a higher amount of total sleep time if compared with AD ones [12]. In addition, some differential elements between DLB, PDD, and AD were highlighted by Oliveira and colleagues, who reported a family history of parkinsonism, low sleep satisfaction, and physical self-maintenance as well as a worse motor performance in PDD if compared to DLB and AD patients. On the contrary, better performance in spatial and calculation tasks was found in AD people [13]. In this framework, recent works suggested that the weakness in visuospatial skills, executive functions, attention, and processing speed are often prodrome symptoms of DLB, while AD was typically associated with impairment in language and memory, delusions, depressive symptoms, aberrant motor behaviours [14,15]. Furthermore, DLB subjects present lower alterations of attention and episodic verbal memory if compared to PDD individuals. However, hallucinations, delusions, and attentional fluctuations are generally more severe in DLB than in PDD [16]. In clinical terms, the risk of hallucinations and dementia, typical signs of DLB, was increased by AD neuropathology, even though no significant relationship was reported between AD neuropathology changes and the risk of hallucinations and dementia [17]. From the other side, the neurocognitive profile of PD patients is sometimes characterized by impairment in executive functions, memory, and visuospatial deficits. About psychiatric symptomatology, anxiety and depression are quite common among PD patients. These symptoms may also lead to frank dementia [18].
In terms of similarities, the above-mentioned diseases have some shared points: both DLB and PDD show executive dysfunctions, visual-constructive and language impairment, mood disturbances such as anxiety and depression, sleep behaviour disorder and a particular sensitivity to neuroleptics [16].
A significant contribution for differential diagnosis between AD, PDD and DLB comes from screening tests. Regarding test accuracy, a study comparing the efficacy of the Montreal Cognitive Assessment (MoCA) and quick Mild Cognitive Impairment (qMCI) found that the latter presented a better accuracy than the MoCA in distinguishing normal cognition from MCI states. Particularly, the qMCI, except from requiring a short administration time, seems to accurately detect early symptoms of dementia [19]. Similarly, the Clock Drawing Test (CDT) is commonly employed to detect early symptoms of dementia [20]. Other tools are the Clinical Dementia Rate (CDR) for dementia assessment, the Neuropsychiatric Inventory Questionnaire (NPI-Q) for neuropsychiatric symptoms, the Geriatric Depression Scale (GDS), and the recent version consisting of 15 items (GDS-15) for depressive symptoms [21–23]. The total Neuropsychiatric Inventory (NPI) score is higher in DLB than in PDD or AD. In the framework of differential diagnosis, the concept of a clinical overlap syndrome should be considered both to better define DLB symptomatology and to suspect it at an earlier stage of the disease [12]. In line with this premise, it seems that subjects with DLB, AD, or PDD may have similar performance at the (CDT), while DLB individuals are more likely to make conceptual errors than AD and PDD patients. Besides, PDD and DLB individuals generally show a higher rate of planning errors compared to AD subjects [24]. A study carried out in AD subjects with & without DLB and assessed by the (CDR) for dementia assessment, the NPI-Q for neuropsychiatric symptoms, the GDS for depressive symptoms, and the Unified Parkinson Disease Rating Scale (UPDRS) motor score for motor problems pointed out that AD and DLB presented higher scores at the NPI-Q and the UPDRS than AD only, thus suggesting a different clinical phenotype for individuals with AD and DLB [25].
In line with these findings and according to existing guidelines, it could be stated that DLB and PDD share a progressive cognitive impairment characterized by parkinsonism, visual hallucinations, and fluctuations of attention and wakefulness.
Finally, diagnostic criteria support evidence of reduced dopamine cell levels detected by single-photon emission computed tomography (SPECT) imaging and for rapid eye movement (REM) together with alterations in sleep pattern in both DLB and PDD [9]. (See Table 1).
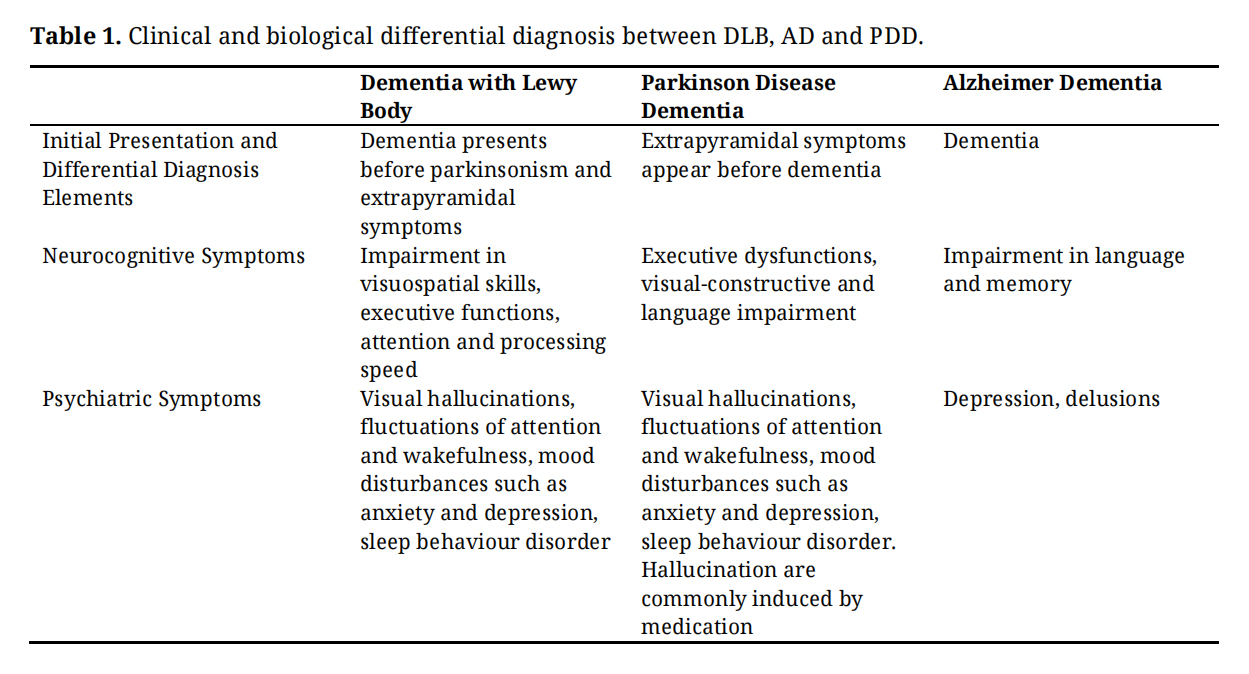 Table 1. Clinical and biological differential diagnosis between DLB, AD and PDD.
Table 1. Clinical and biological differential diagnosis between DLB, AD and PDD.
Stimulating evidence of a common genetic basis between PD and AD seems to come from a genome-wide meta-analysis by Real et al. (2023) who identified APOE-4 as a major risk factor both for AD and for the conversion from PD to PDD [26]. Accordingly, a recent study by Wu et al. (2024) confirmed the causative role of APOE-4 for the development of dementia, while SNCA-AS1 and LKKR2 seem to exert a protective role [27]. Regarding SNCB, it has been reported a high prevalence of genotypes associated with low gene expression [28]. In support of this evidence, Guerreiro and colleagues suggested that DLB and PD share lots of genetic determinants, the APOE locus [29]. Another shared genetic polymorphism is 5HTTLPR, a 43-base-pair insertion/deletion in the promoter region of the SLC6A4, with a short and long allele, often associated with delusions in DLB [30]. In this framework, a study carried out in individuals with DLB and PDD found that those with homozygosis for the L/L genotype and a lower Mini Mental State Examination (MMSE) score showed an increased risk for delusions, thus suggesting that the 5HTTLPR polymorphism is associated with delusions in DLB [30]. Accordingly, Quaranta et al. (2009) and Sweet and colleagues reported the L/L genotype to be associated with psychosis in AD and, in turn, suggested that the 5-HTTLPR polymorphism might be a shared risk factor for psychotic symptoms across diseases [31,32]. Other genes implicated in the pathophysiology of AD, PD, and DLB, are glucocerebrosidase gene (GBA) variants, the SNPs, which could be useful target therapeutic interventions [33,34], and the microtubule-associated protein tau gene (MAPT), that may be associated with the risk of DLB and PDD [16]. When analysing DNA methylation patterns among different neuropsychiatric disorders, Fisher et al. (2023) pointed out that DLB and PD differed in the level of methylation in 197 regions with PD being associated with hypomethylation [35]. However, it should be considered that there have been conflicting results on the association between this polymorphism with a variety of neuropsychiatric symptoms and syndromes, also giving the fact that many of these studies are too small [36] (See Figure 2).
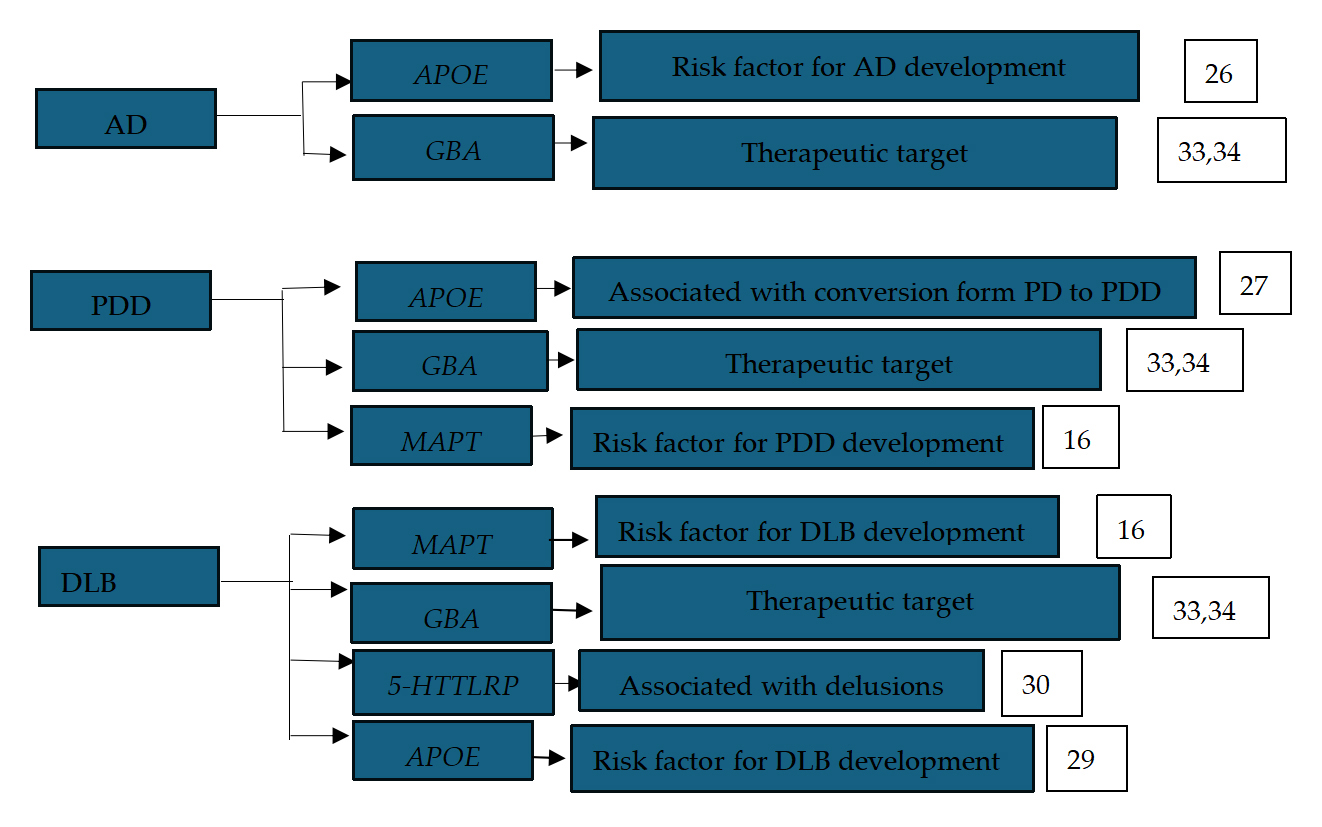 Figure 2. Main genes implicated in AD, PDD and DLB. References numbers are reported in the box.
Figure 2. Main genes implicated in AD, PDD and DLB. References numbers are reported in the box.
DLB and PD are characterized by the accumulation of aggregated α-syn protein, while AD is also frequently accompanied by aggregation of amyloid-beta and tau [3]. However, the overexpression of β-amyloid peptides and of interleukin-1 (IL-1) as well as the α-syn accumulation are often considered a common feature of AD, PDD, and DLB. Specifically, it seems that α-syn accumulation and its related neuron pathology may be facilitated by beta-amyloid peptides. Besides, neuropathological changes are sometimes driven by glial activation together with IL-1 level alterations [37,38]. Jellinger et al. (2018) considered PDD, DLB, and AD as part of the same α-synuclein-associated disease spectrum [16]. However, it should also be considered that each disease is related to different synucleinopathy processes and that cognitive alterations may be explained not only by α-synuclein-related neurodegeneration but also with multiple regional pathological affection [16,39,40]. Intriguingly, recent evidence reports a sex difference for neuropsychiatric symptoms across alpha-synucleinopathies, with males being associated with a higher prevalence of apathy, impulse control disorders, sleep problems, and suicide, while females generally exhibit anxiety, depression, fatigue, and psychotic symptoms [41].
Molecular contribution to differential diagnosis between dementia in AD and in PDD also comes from studies combining NPI scores with biological elements. Specifically, the combination of NPI score with α-syn levels predicted the inclusion in the DLB group instead of in PDD or AD [39,42]. Interestingly, α-syn accumulation may be at the basis of anxiety and depression, found both in PDD and in DLB. Moreover, compared to PDD individuals, those with DLB showed the greatest amount of functional impairment at the activities of daily life [43]. An interesting staging system for DLB is that proposed by Braak, who associated severe LB pathology and PD with severe neuropathological changes [44]. Also, sphingolipids and phospholipids seem to be significantly altered in DLB. What’s more, the lipid profile may be an effective biomarker for differential diagnosis between DLB and AD [45]. Meantime, some authors reported higher levels of synuclein aggregates in DLB individuals compared to AD patients, who, in turn, had more elevated glial-associated matrisome signatures [46].
Interestingly, it was found a significant correlation between the presence of the APOE ε4 aggregates and a higher cortical LB load in the temporal and parietal regions from the one side and a shorter latency to dementia from the other [47].
In this framework, also cerebrospinal fluid (CSF) analysis suggests that DLB, AD, and PDD may be differentiated based on different protein levels. In fact, PDD individuals generally show lower CSF amyloid β42 (Aβ 42) levels than those with Parkinson’s disease without dementia [48]. In addition, Aβ 42 CSF levels tend to decrease in DLB from early states to moderate and severe ones [49]. Methoxy-4-hydroxyphenylethyleneglycol (MHPG) CSF levels, together with those of t-tau, p-tau, and A-42 proteins, have been presented as a potential DLB biomarker [50]. Instead, AD is associated with significant levels of CSF T-Tau and pTau181 if compared to DLB and PDD. However, P and Tau levels seem to correlate with disease severity in both AD and DLB, with higher protein levels found in more severe states [49]. Furthermore, it was found an association between CSF-derived biomarkers of Aβ42, t-tau/Aβ42 and depressive symptoms in subjects with both DLB and AD [51].
Other molecular mechanisms implicated in PDD are the loss of limbic and cortically projecting dopaminergic neurons in the mesocortical limbic system and an alteration in the cholinergic system, namely in the nucleus basalis of Meynert [52–54] (See Figure 3).
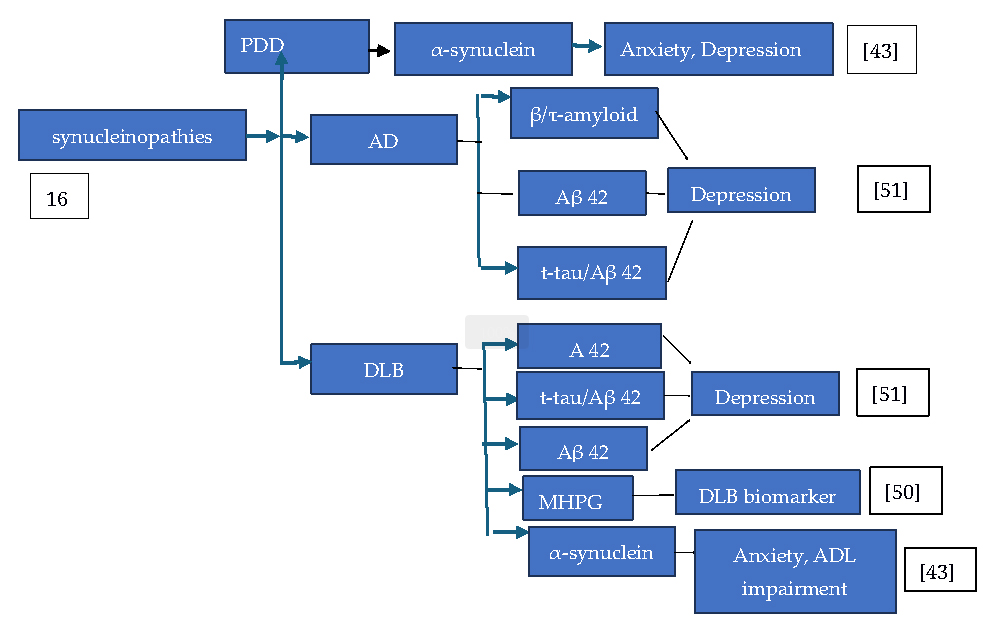 Figure 3. Proteins accumulations and neuropsychiatric symptoms in AD, DLB and PDD. Abbreviations: ADL: activities of daily life. References numbers are reported in the box.
Figure 3. Proteins accumulations and neuropsychiatric symptoms in AD, DLB and PDD. Abbreviations: ADL: activities of daily life. References numbers are reported in the box.
Some works report a cortical thinning, especially in entorhinal and parahippocampal regions, for AD and DLB. Moreover, DLB subjects have been reported to have their medial temporal lobe structures more preserved than those with AD, and, as for PDD individuals to generally show less cortical thinning [6]. From the other side, AD is associated with regional thinning in the medial temporal and temporoparietal cortices as well as in the frontal lobes [55–57].
From a wider point of view, it seems that DLB patients show more pronounced cortical atrophy than PDD individuals. In fact, post-mortem studies reveal a pronounced cortical atrophy and diffuse cortical and limbic alterations in DLB with respect to PDD. In turn, these findings could justify the earlier onset and greater severity of cognitive defects in DLB [9]. Furthermore, cortical atrophy in DLB typically regards medial, ventral, and ventrolateral temporal cortex [6,55,57]. About hippocampal regions, alterations of cornu ammonis, associated with memory function, are more frequent in AD than in PDD and DLB [58]. DLB is also associated with atrophy in striatum regions including caudate, putamen, and pallidum [59,60]. Besides, DLB patients exhibit a homogenous pattern of brain stem atrophy that can be distinguished from PDD subjects [61].
When analysing different brain networks in DLB, PDD, and AD, the former presented the lowest level of global and local efficiency [62]. Moreover, gray matter cortical atrophy seems more frequent and severe in DLB than in PDD [16]. Similarly, Cerebral amyloid angiopathy (CAA) seems to be typical of DLB, with significantly higher scores in the parietal and occipital lobe. Interestingly, CAA and a rapid disease progression have been suggested as potential biomarkers to distinguish DLB from PDD [63] (See Figure 4).
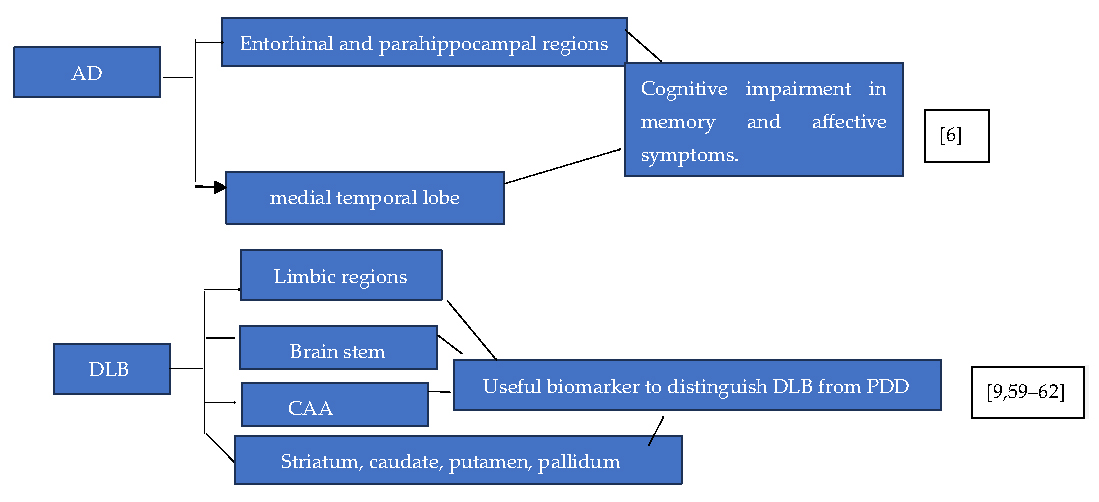 Figure 4. Cerebral regions atrophy in AD and DLB: clinical correlates. References numbers are reported in the box.
Figure 4. Cerebral regions atrophy in AD and DLB: clinical correlates. References numbers are reported in the box.
Regarding electrophysiological aspects, DLB is associated with a decreased dominant frequency. In this framework, Peraza and colleagues assessed the brain network by the minimum spanning tree (MST) finding a randomized MST in DLB and PDD patients if compared with HCs and AD individuals and thus suggesting a decreased brain efficiency and an altered neural synchronization in the formers [64].
About instrumental exams, a recent meta-analysis focused on mild cognitive impairment diagnosis in Lewy Body Disease (MCI-LB) showed that electroencephalogram (EEG) and fluorodeoxyglucose PET may be important tools for this clinical situation [65]. Specifically, PDD individuals presented abnormalities in EEG [66]. Furthermore, for MCI-LB patients, PET reported a posterior cerebral hypometabolism and hypoperfusion when compared with Mild cognitive impairment in Alzheimer Disease (MCI-AD) and controls, while EEG slowing was associated with visual hallucinations and poorer cognitive performance in MCI-LB [65]. Thanks to amyloid positron emission tomography and dopamine transporter single photon emission computed tomography (DAT-SPECT) analysis, it has been pointed out that the presence of amyloid and putative Lewy Body pathologies was associated with psychotic symptomatology [40]. It should also be considered that both DLB and PDD present similar metabolic patterns of reduced metabolism in parietal, frontal, anterior cingulate, and occipital regions if compared to healthy controls [67,68]. Moreover, DLB metabolic pattern underlying cognitive impairment, even though not detrimental for general survival, seems to be like that of AD [69]. Besides, metabolism in the posterior cingulate gyrus is particularly useful to make a differential diagnosis between DLB and AD. In fact, DLB is associated with hypermetabolism in the posterior cingulate if compared to the precuneus and cuneus. From the other side, hypometabolism in AD mainly affects temporal, parietal and frontal regions [70]. Intriguingly, functional impairment in motor-related regions, as shown by regional homogeneity (ReHo) studies, suggests that there exists a Lewy body disease spectrum of alterations. ReHo differences among the diseases, such as the default mode networks (DMN) and sensory-motor resting state networks, could be at the basis of aetiological divergences between AD and DLB [64]. DMN studies, in fact, revealed that, compared to PD and DLB subjects, AD patients present a significant reduction in the posterior cingulate cortex activity. Meanwhile, DLB and PDD are characterized by impairment in the posterior brain regions, namely the occipital, parietal, and precuneal cortices [71]. To be accurate, it could be stated that while PDD is associated with frontal cortical disruption, DLB is characterized by parietal and occipital impairment [16]. Regarding sensory motor network abnormalities, functional connectivity alterations of the basal ganglia and cortical motor regions have been reported in DLB [3]. By combining another functional measure, the SN, with the central executive network (CEN) it could be found that are more common in DLB than in AD [16]. Another useful functional tool to detect dementia affecting older individuals is white matter hyperintensity (WMH), usually associated with cortical thinning and cerebral atrophy [72]. WMH alteration pattern seems to be more severe in DLB and AD than in PD dementia. Hyperintensity is more severe in the temporal lobe in DLB than in PD dementia [16] (See Figure 5).
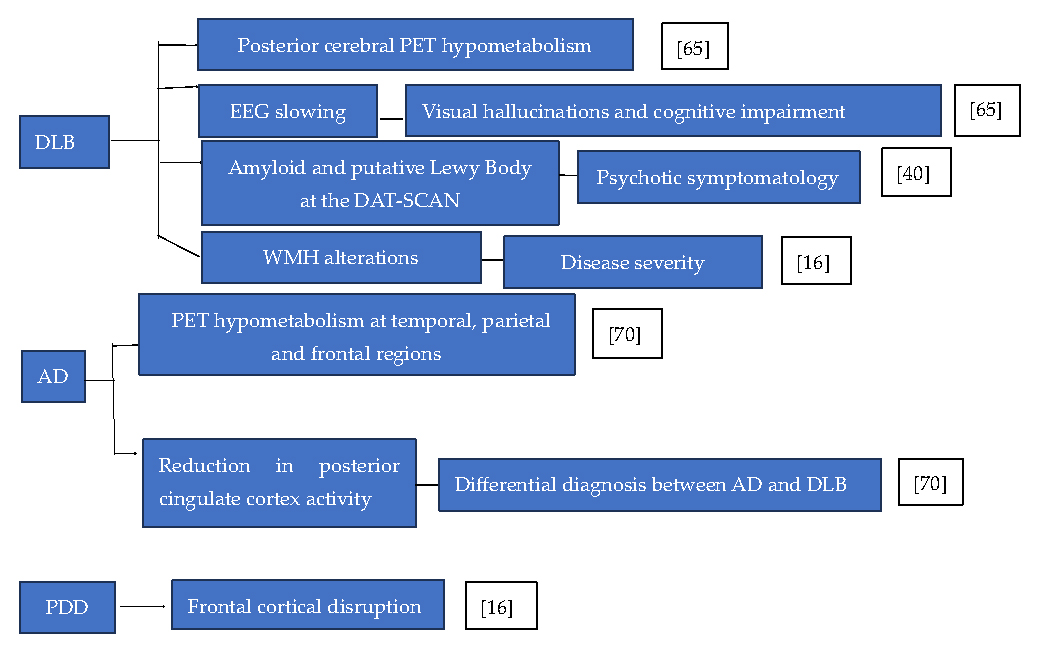 Figure 5. Association between metabolic alterations and neuropsychiatric conditions in AD, PDD and DLB. Abbreviations: DAT-SCAN: dopamine transporter single photon emission computed tomography. References numbers are reported in the box.
Figure 5. Association between metabolic alterations and neuropsychiatric conditions in AD, PDD and DLB. Abbreviations: DAT-SCAN: dopamine transporter single photon emission computed tomography. References numbers are reported in the box.
To date, no resolutive therapy is currently available for these disorders. To target depressive symptoms, daytime somnolence, agitation, insomnia, anxiety, dysautonomia, urinary incontinence, and constipation, different pharmacological strategies have been proposed, while no univocal efficacy has been reported for the same drugs [9].
For neuropsychiatric aspects of parkinsonism, the only antipsychotic unequivocally associated with hallucinations improvement is clozapine. Among the antipsychotics, also quetiapine is associated with less worsening of Parkinson symptomatology [73]. However, acetylcholinesterase inhibitors (ChEI) also seem to partially ameliorate the psychotic symptoms of PD [44]. In addition, ChEI are reported to reduce apathy, visual hallucinations, and delusions, especially in DLB and PDD [74]. For psychosis in AD, some data suggest the usefulness of typical antipsychotics in decreasing agitation and psychosis, while atypical antipsychotics seem to reduce agitations with a mild effect on psychosis [75]. Moreover, a review has highlighted the potential utility of lithium and other mood stabilizers in managing mixed-manic symptomatology in patients with dementia [76], as further supported by clinical observations from low-dose lithium treatment for agitation and psychosis in AD and frontotemporal dementia [77]. Carbidopa/levodopa have shown some benefits for psychomotor slowing in DLB and PDD [9].
According to British guidelines, similar drugs should be employed for treatment of dementia in PD and DLB. The three available cholinesterase inhibitors, donepezil, rivastigmine and galantamine, show promising results on cognitive symptoms of the diseases and sleep, with mild cholinergic side effects including nausea, vomiting, anorexia, and somnolence. Particularly, donepezil and rivastigmine have been employed for dementia in PD with comparable effects to AD. Some good effects have been reported for L-DOPA and DA agonists in neuropsychiatric symptoms of PD [18]. For depressive and anxiety symptoms, Selective Serotonin Reuptake Inhibitors (SSRI) and Serotonin Noradrenaline Reuptake Inhibitors (SNRI) appear to be the preferred pharmacological treatments, while for REM sleep behavior disorder, it could be recommended to take clonazepam at bedtime. Daytime somnolence may be improved by coffee, methylphenidate, amphetamine, and modafinil, while agitation could benefit from quetiapine and clozapine [9,78]. Disease-modifying drugs, as shown by recent vaccination trials against αSyn, Aβ, and tau proteins, are promising therapeutic strategies to target neuropsychiatric symptoms of AD, PDD and DLB [79,80]. Among New Disease Modifing Drugs in AD, there are anti-amyloid and anti-tau therapies that could be useful therapeutic approaches both for cognitive and behavioral symptoms of AD [81,82]. In addition, lithium has demonstrated neuroprotective properties in both preclinical [83] and clinical studies [84], particularly through its inhibition of glycogen synthase kinase-3β (GSK-3β) and its effect on tau phosphorylation. However, its clinical efficacy in AD remains under investigation. Recently, a retrospective case series of 7 patients with DLB suggested the Ultrabrief Right Unilateral Electroconvulsive Therapy (UB RUL ECT) for the treatment of agitation and depressive symptoms in individuals with DLB [85]. Furthermore, ECT has also proven effective in treating catatonia associated with psychiatric symptoms in patients with Parkinson’s disease and comorbid psychosis, as reported in a case where it was administered in a patient with PD and psychosis [86]. Similarly, a work by Elefante et al. (2022) specifically addressed catatonia in the context of PD and affective episodes. The authors reported that ECT was effective to treat catatonic symptoms without cognitive worsening [87] (See Table 2).
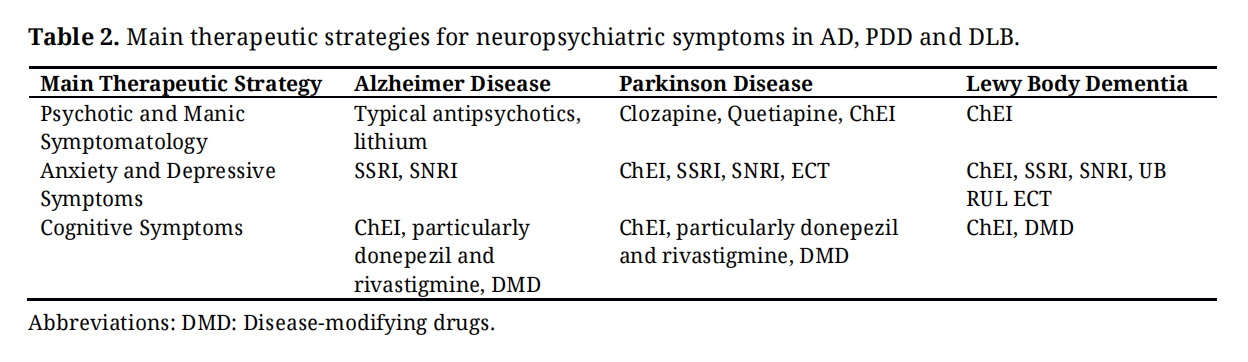 Table 2. Main therapeutic strategies for neuropsychiatric symptoms in AD, PDD and DLB.
Table 2. Main therapeutic strategies for neuropsychiatric symptoms in AD, PDD and DLB.
This work reviews the current literature dealing with genetic, molecular, anatomical, and electrophysiological correlates of neuropsychiatric symptoms shared across AD, PDD, and DLB. The main genetic alterations discussed in the present review are: APOE-4, which is also a risk factor for the development of PDD [26], 5HTTLPR, often associated with delusions in DLB [30], MAPT, which positively correlates with the development of DLB and PDD [16], and GBA variants, which could also be promising therapeutic targets for AD, PDD, and DLB [33,34]. In this framework, Wightman and colleagues reported 2 genetic loci, namely TMEM175 and HLA, shared across the diseases. Moreover, the authors pointed out some other genes, implicated in the inflammatory processes and found to be altered both in DLB and AD: CSF1, TYROBP, and TREM2 [88]. Particular attention has been paid by Olney et al (2025) to the upregulation of SPP1, CSF1, TYROBP and TREM2 in the pathophysiology of DLB [89].
When dealing about molecular common basis underlying different pathologies, α-synuclein and β/τ-amyloid accumulations were reported as the most significant, the first being associated with PDD and DLB and the second with AD [39,42]. Specifically, t-tau and Aβ 42 levels were significantly associated with depressive symptoms of both AD and DLB [43]. In this framework, Sengupta and colleagues suggested that Aβ and tau pathology usually co-exist in AD, PDD, and DLB [90]. Partially in contrast with this evidence, Jellinger (2022) reported that Aβ plaques as well as CAA deposits were more common in DLB than in PDD, thus justifying a worse prognosis for DLB patients [91]. In addition, intriguing findings on molecular correlates shared across the diseases seem to come from similar microglial activation in AD and PDD. In fact, it was pointed out that microglia activation, also in response to TREM2 increased expression, could lead to the spread of pathologically misfolded proteins that, in turn, could exert a toxic effect both in DLB and AD. Besides, it seems that the impairment of the vascular endothelial growth factor signaling could alter the integrity of blood-brain barrier. Finally, the downregulation of synaptic signaling, as well as of behavior and neuronal systems have been found as a characteristic of both DLB and AD [89].
From an anatomical point of view, temporal regions were found to be frequently altered in AD, while the impairment of limbic, hippocampal, caudate and brain stem regions positively correlated with severity of PDD and DLB [55–61].
About functional and neurophysiological mechanisms, WMA seem to be typical of both AD and DLB [71]. In terms of differences, MCI-LB individuals showed a posterior cerebral hypometabolism and hypoperfusion, while EEG slowing together with delusions and hallucinations are frequently found in DLB [65]. Meanwhile, PET hypometabolism in temporal, frontal and parietal regions was also related to AD [70]. Renewed interest about neuroimaging correlates of AD, PDD, and DLB has recently grown, as shown by the several trials active to find out PET imaging tracers for neuroinflammation [90].
Dealing about therapeutic perspectives, antidepressants, such as SSRI and SNRI could be useful to target anxiety and depression in the above-mentioned disease, while antipsychotics may have a rationale to target delusions and hallucinations [73,75,78]. Even ChEI, commonly employed for cognitive symptoms of neurodegenerative diseases, could play a role for behavioral aspects of AD, PDD, and DLB [74].
It should also be noted that many of the pharmacologic treatments used to treat behavioral and cognitive symptoms in other forms of dementia may exacerbate the symptoms of DLB and even death. In fact, Mausted and colleagues reported a significant increase of mortality in individuals taking typical haloperidol and atypical antipsychotics, namely olanzapine, quetiapine and risperidone [92]. Another frequent adverse event of psychotropic drugs in older age is delirium. Anticholinergic drugs, anticonvulsants, histamine H2 receptor antagonists and particularly long-acting benzodiazepines are commonly implicated in delirium in the elderly. Polypharmacy avoidance, specific attention in prescribing drugs, and early diagnosis of drug-induced confusion could be very useful for preventing delirium in geriatric ages [93]. Conversely, a work by Ramm and colleagues seems to report some benefit from delta-9-tetrahydrocannabinol (THC) as alternative to antipsychotic drugs for behavioral symptoms of dementia [94]. Another promising therapeutic strategy to address psychotic symptoms comes from pimavanserin, which has been proven as a well-tolerated drug for neuropsychiatric symptoms of neurodegenerative diseases [95].
Promising results also come from disease modifing drugs including vaccinations against αSyn, Aβ, and tau proteins. Among disease modifying drugs, encouraging findings have been highlighted for combinatorial therapeutics such as the antibody crenezumab, that targets both Aβ and tau proteins. The utility of combination therapies could be explained by their synergistic or additive effects, useful for both AD, PDD, and DLB. Accordingly, promising strategies could consist of antibodies specifically targeting multi-protein aggregates implicated in the pathophysiology of the above-mentioned diseases [90].
Overall, it could be stated that AD, PDD, and DLB share genetic, molecular, biological, and electrophysiological elements. Meanwhile, these aspects could be helpful to make proper differential diagnosis. In this framework, Jellinger and Korczyn suggested extensive multidisciplinary studies to identify genetic and environmental risk factors and ameliorate the understanding of the biological mechanisms underlying the mentioned diseases [16]. Intriguingly, clinical manifestations of the diseases and diagnostic findings specific to each pathology may be correlated with known pathophysiology. Finally, the fact that neuropsychiatric symptoms of these diseases could be approached by common therapeutic strategies could potentially suggest, another time, a common pathogenetic basis.
Not applicable.
Not applicable.
No data was generated from the study.
The author declares that he has no conflicts of interest.
This review did not receive any funding.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
68.
69.
70.
71.
72.
73.
74.
75.
76.
77.
78.
79.
80.
81.
82.
83.
84.
85.
86.
87.
88.
89.
90.
91.
92.
93.
94.
95.
Massoni L. Neuropsychiatric symptoms of Alzheimer disease, Parkinson disease and Lewy body dementia: Genetic, clinical and therapeutic overlaps. Adv Geriatr Med Res. 2025;7(3):e250013. https://doi.org/10.20900/agmr20250013.

Copyright © Hapres Co., Ltd. Privacy Policy | Terms and Conditions




