Location:Home >> Detail
J Psychiatry Brain Sci. 2017; 2(5): 2; https://doi.org/10.20900/jpbs.20170016
 ,
Hui Xiang1 ,
Qing Qin1,
Ying Huang1 ,
Zhenggui Yang1 ,
Maolan Zhang1
,
Hui Xiang1 ,
Qing Qin1,
Ying Huang1 ,
Zhenggui Yang1 ,
Maolan Zhang1
1 Guizhou Provincial People’s Hospital, Guizhou, Guiyang 550002, China
*Correspondence: Hui Yang.
Objective: To explore the clinical efficacy of right low frequency repetitive transcranial magnetic stimulation (rTMS) therapy combined with escitalopram in treating outpatients with first-episode depression.
Methods: Seventy-eight patients with depressive disorder of ICD-10 criteria were recruited for the trial. All subjects were randomly divided into the active rTMS group (receive active rTMS) and sham group (receive sham rTMS). Each group received low frequency active or sham rTMS combined with 10 mg escitalopram per day. Patients in the active rTMS group were treated with active rTMS for continuous two weeks, while the sham patients were treated with pseudo stimulation. HAMD, HAMA and TESS were used to assess the efficacy and side effects before the treatment and at the ends of the second week and the fourth week of treatment, respectively.
Results: 1) At the end of 4 weeks’ treatment, patients in the active rTMS group had a response rate of 87.8 % while the patients in the sham group had 41.5 %; 2) patients in the active rTMS group showed a significant efficacy at the end of 2 weeks, which was significantly different from the patients in the sham group; 3) Patients in the active rTMS group got a significantly lower score in HAMA at the end of 2 weeks, and there was a significant difference from the sham group; 4) There was only a local pain response.
Conclusion: The right low-frequency rTMS technique combined with escitalopram in treatment of depressive patients in general hospitals has a significant better effect than mono-pharmacotherapy and can shorten the time of treatment.
The repetitive Transcranial Magnetic Stimulation (rTMS), a safe, noninvasive and painless nerve stimulation technique that has been applied in the field of neuropsychiatry in recent years, showed a reliable effect on neuropsychiatric disorders[1]. At present, a large number of clinical trials have confirmed that the efficacy of treating the depressive disorder using high frequency rTMS to stimulate dorsolateral prefrontal cortex (DLPFC) at right brain has been widely recognized[2, 3]. However, there are fewer studies on treatment of depressive patients using the right low frequency rTMS technique to stimulate DLPFC. This study aims to explore the early clinical efficacy and side-effect impact of right low frequency repetitive transcranial magnetic stimulation (rTMS) therapy combined with escitalopram in treating outpatients with first-episode depression in general hospitals.
Eighty-two outpatients with first-episode depression were recruited from the psychology department of the People’s Hospital of Guizhou Province from August 2016 to March 2017, 78 of which finally completed this study. The relevant information of the 78 outpatients was listed here. Inclusion criteria: a. all subjects conformed to the psycholepsy diagnosis criteria of ICD-10 Mental and Behavioral Disorders; b. aged 18-60 years old; c. first-episode depression and no administration of any antidepressants and antipsychotic drug. Exclusion criteria: a. patients with severe physical illness or brain organic diseases; b. patients with depression caused by psychoactive substances and non-dependent substances; c. patients with an implanted metal object or cochlear; d. patients previously treated with rTMS; e. patients with severe epilepsy; and f. patients with risk of suicide.
Each subject or his / her family member signed the informed consent. There were 17 male patients and 24 female patients in the active rTMS group, aged 35.5 ± 12.0 years old, and there was 1 patient with postgraduate education, 20 patients with undergraduate or college education, 15 patients with senior high school or secondary technical school education, 4 patients with junior high school education and 1 patient with primary school education or below. There were 16 male patients and 25 female patients in the sham group, aged 35.4 ± 12.1 years old, and there were 2 patients with postgraduate education, 18 patients with undergraduate or college education, 18 patients with senior high school or secondary technical school education, and 3 patients with primary school education or below. The difference of the above general demographic characteristics was not statistically significant between the two groups (p > 0.05), see Table 1. for details.
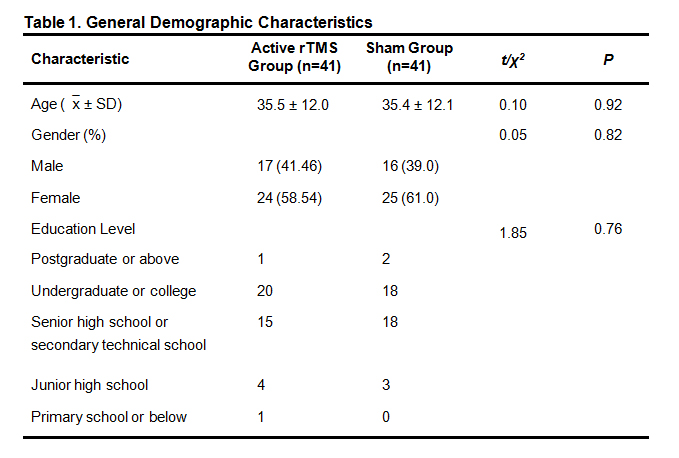 Table 1. General Demographic Characteristics
Table 1. General Demographic Characteristics
The research method of randomized controls was used to divide the 82 subjects into the active rTMS group and sham group using the random number table method. YRD CCY-1 transcranial magnetic stimulation instrument was used. 1Hz and 100 % exercise threshold value was used in the active rTMS group to stimulate the right prefrontal lobe lateral area. The total number of each stimulus pulse was 1200 and total stimulation time was 20 minutes, and the continuous treatment time was 10 work days. The pseudo-stimulated therapy was used in the sham group (the angle between stimulus coil and scalp was 90 degrees or 45 degrees, and no effective magnetic field was provided to it), and the stimulation intensity, frequency and times were the same as those in the active rTMS group. During the study period, all subjects were treated with escitalopram, 10 mg/d (specification: 10 mg/tablet).
1.2.2 Assessment toolsHAMD-17, HAMA and TESS were used to assess the clinical efficacy and side effects. The scale assessment was made by 4-5 specially trained psychiatrists and the consistent test was also made. The assessment was made before the treatment, and at the ends of the second week and fourth week of treatment, respectively; the score-reducing rate was used to assess the clinical efficacy: it was regarded as effective when score-reducing rate ≥ 50 %. TESS was used to assess the safety. The maximum score of all items that was equal to or greater than 2 points after the treatment was regarded as adverse reaction.
1.2.3 Statistical analysisAll information or data were recorded and analyzed using software SPSS16.0, and the relevant information was compared using the methods of χ2 test, t test and variance analysis.
A total of 82 patients were included in this study, including a dropout case due to a limited time, two dropout cases due to pain at the stimulated site in the active rTMS group, and one dropout case due to pain at the stimulated site in the sham group. There were 78 subjects who actually completed the study, accounting for 95 % of the total number of recruited patients. When the efficacy indicators were counted, the Last Assessment Carry Forward (LACF) was used to count the relevant scale scores of the dropout cases.
2.1 Comparison of Clinical EfficacyAfter four-week treatment, there were 36 effective cases in the active rTMS group, with an effective rate of 87.8 %, and there were 17 effective cases in the sham group, with an effective rate of 41.5 %. The difference of effective rates between the two groups was statistically significant (χ2 = 19.26, p < 0.05).
2.2 Comparison of HAMD-17 ScoresThe studies showed that the HAMD-17 score of the active rTMS group at the end of 2-week treatment was reduced with a statistical significance (F =118.53, p = 0.00) and the difference of HAMD-17 score of the active rTMS group at the end of 2-week treatment from the same period score of the sham group was statistically significant (t = 6.19, p = 0.00). The HAMD-17 score of the active rTMS group was significantly lower than that of the sham group. Compared with the score of baseline period, the score of the sham group at the end of the second week of treatment was not reduced with a statistical significance. Compared with the score of baseline period at the end of the fourth week of treatment, the difference between the two groups was statistically significant (p < 0.01), see Table 2.
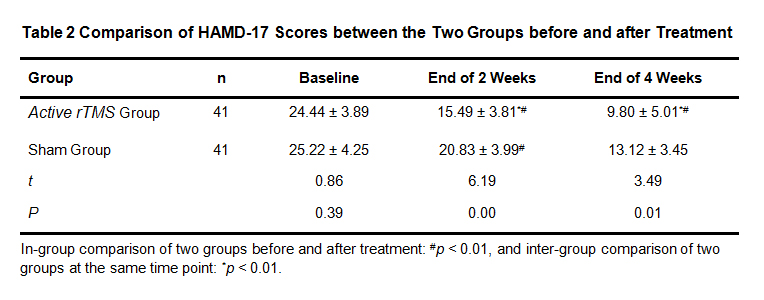 Table 2 Comparison of HAMD-17 Scores between the Two Groups before and after Treatment
Table 2 Comparison of HAMD-17 Scores between the Two Groups before and after Treatment
After the treatment, HAMA score of the active rTMS group was significantly reduced at the ends of both week 2 and week 4 and the difference was statistically significant (p < 0.01), see Table 3.
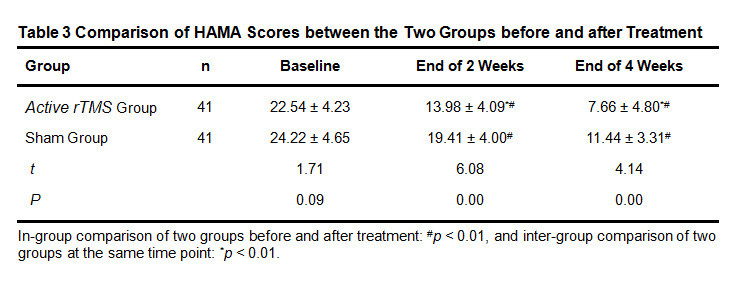 Table 3 Comparison of HAMA Scores between the Two Groups before and after Treatment
Table 3 Comparison of HAMA Scores between the Two Groups before and after Treatment
No severe adverse reaction was occurred during the study period among the subjects of two groups. There were two cases of scalp pain and dizziness in the active rTMS group, but they were self-mitigated without treatment. There was no tinnitus, convulsion or other adverse reaction in both groups.
The depressive disorder has a high prevalence, high recurrence rate, high disability and high suicide rate. In recent years, a significant progress has been made in the study on the treatment of depressive disorder using the rTMS treatment technique. The studies of cerebral cortical function showed that, for a bilateral DLPFC dysfunction of depressive patients, the left DLPFC involved in the generation and regulation of positive emotions and the right DLPFC involved in the generation and regulation of negative emotions, while the left DLPFC function of depressive patients was abnormally weakened and the right DLPFC function was abnormally enhanced. The emotional disorder of patients can be improved by improving the patients’ DLPFC functions[4-6]. The outpatients of psychology department/psychiatry department of general hospitals are mostly patients with anxiety and depression. It has been reported that 63.8 - 90.1 % of the depressive patients who have been diagnosed and treated in psychiatry department paid their first visit to the general hospitals[7]. At present, antidepressant effect is slow, the drug side effect at the initial stage of treatment is obvious, and the treatment cost is very high. All of those cause a poor medication compliance of the patients. If the outpatient doctors can control the acute symptoms in a faster and better way, it will help improve the patients’ treatment compliance. Moreover, a rapid effect and early cure can also have a better predictive effect on prognosis [8]. Hence, the improvement of early treatment efficacy in patients with first-episode depression will help fully cure the patients and reduce the complexity and refractoriness of the diseases. In the past, rTMS treatment techniques were mostly concentrated on the left high frequency studies. Compared with the left high frequency stimulation therapy, studies suggest that, the right low-frequency rTMS treatment technique is not easy to induce the convulsions relative to the high frequency stimulation, and it is of a lower risk and better tolerance and it may be the best treatment method[6, 9]. The right low-frequency rTMS treatment method was used in this study.
The results of this study showed that HAMD-17 score and HAMA score of the active rTMS group were significantly lower than that of the sham group at the end of the second week of treatment, suggesting a faster effect time and better efficacy for the right low-frequency rTMS technique combined with escitalopram in treatment of depressive patients compared with the treatment only using the escitalopram. This is consistent with the existing studies at home and abroad[10-12]. At the end of the fourth week of treatment, the difference of HAMD-17 scores and HAMA scores between two groups compared with those before the treatment was statistically significant (p < 0.01), suggesting that either the treatment only with escitalopram or the right low-frequency rTMS technique combined with escitalopram in treatment of patients with first-episode depression can effectively improve the anxiety and depression symptoms of the patients. Moreover, at the ends of the second week and fourth week of the treatment, HAMD-17 and HAMA scores of the active rTMS group were significantly lower than the same period data of the sham group, suggesting that the efficacy advantage of the right low-frequency rTMS technique combined with escitalopram in treatment of patients with first-episode depression over the treatment of the patients only using the escitalopram was maintained two weeks after the termination of the right low-frequency rTMS treatment technique.
Furthermore, there was no epilepsy, convulsion or other severe adverse reaction in all subjects in this study, and there was a good safety during the treatment period. Compared with the adverse reaction of the sham group, the difference was not statistically significant. It is noteworthy that, some studies showed that, compared with the high-frequency magnetic stimulation of left brain dorsolateral prefrontal cortex in treatment of depressive patients, the patients were more tolerant of the right low frequency rTMS therapy. This suggests that the rTMS therapy method used in this study is worthy of promotion.
In summary, this study shows that, the antidepressants combined with the right low frequency rTMS technique can significantly shorten the effect time and enhance the efficacy of antidepressants and effectively mitigate the patients’ anxiety and improve the treatment compliance of the patients. It has a good safety and applies to the non-hospitalized depressive patients.
Due to restrictions of time conditions, treatment equipment and personnel lack, the study sample was relatively small and observation time was short. In the follow-up studies, we will try the best to increase the number of samples and extend the observation period after treatment so as to draw a more convincing conclusion.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
Yang H, Xiang H, Qin Q, Huang Y, Yang Z, Zhang M. A Randomized Controlled Trial of Right Low Frequency rTMS Combined with Escitalopram in Treatment of Patients with First-episode Depression in General Hospitals. J Psychiatry Brain Sci. 2017; 2(5): 2; https://doi.org/10.20900/jpbs.20170016

Copyright © 2020 Hapres Co., Ltd. Privacy Policy | Terms and Conditions




