Location:Home >> Detail
Med One. 2018; 3: e180013. https://doi.org/10.20900/mo.20180013

Diabetes Centre, Second Department of Internal Medicine, Democritus University of Thrace, University Hospital of Alexandroupolis, Dragana, Alexandroupolis 68100, Greece.
Corresponding Author: Nikolaos Papanas.
During the last decades, there has been a huge increase in the prevalence of type 2 diabetes mellitus (T2DM), mostly due to the Western lifestyle [1,2]. T2DM and its vascular complications increase patient morbidity, hospitalisations and healthcare costs [3,4]. Thus, it is beyond doubt that we need medication which can confer some improvement in the underlying pathophysiological factors leading to T2DM and its complications.
Glucagon-like peptide 1 receptor agonists (GLP-1RAs) are a class of antidiabetic agents, which was introduced in the 21st century. They successfully target not only blood glucose control but also obesity in patients with T2DM [5,6]. Currently, exenatide, liraglutide, lixisenatide, albiglutide and dulaglutide are already on the market [5,7]. The newest agent is semaglutide [5–7].
All GLP-1RAs are used subcutaneously. Albiglutide, dulaglutide and semaglutide show a long action and are administered once weekly [6,8–11]. Liraglutide is used once daily. Exenatide exists in two preparations: a quick acting used twice per day, and a long-acting used once per week [6,8–11]. An oral form of semaglutide is currently under development [6,8–11].
GLP-1 RAs mainly act by activating the GLP-1 receptors in pancreatic beta cells to stimulate glucose-dependent insulin secretion. Additionally, they reduce appetite and delay gastric emptying, eventually leading to reduced food intake [6,8–10]. They can be used either as monotherapy or an add-on therapy to other antidiabetic agents, including insulin, in T2DM [11–13]. GLP-1RAs have very recently been recommended as the second antidiabetic agent after metformin in patients with established atherosclerotic cardiovascular disease and chronic kidney disease [14]. However, they should not be used together with dipeptidyl peptidase-4 inhibitors [10–13]. As regards type 1 diabetes mellitus, they have been studied but they are not currently approved [9,11,13].
The advantages of GLP-1RAs include: (a) efficacy (reduction of glycated haemoglobin 0.6–1.9% in a period of 24–30 weeks); (b) absence of hypoglycaemias; (c) weight reduction; (d) reduction of appetite; (e) reduction of fatty liver infiltration. These actions are significant and clinically meaningful (see Table 1) [5,10,11–13,15,16].
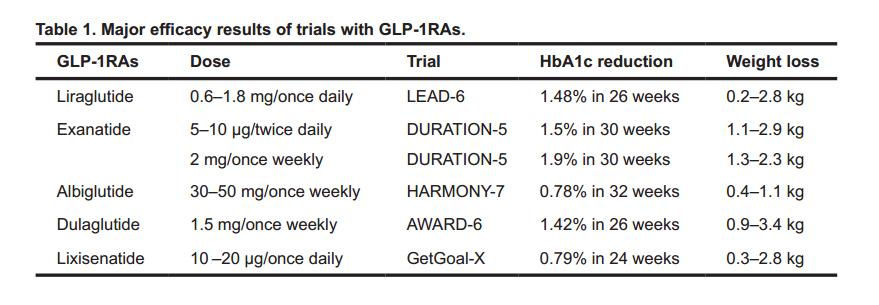 Table 1. Major efficacy results of trials with GLP-1RAs.
Table 1. Major efficacy results of trials with GLP-1RAs.
Regarding their combination with other antidiabetic agents, there are interesting results from some trials. In a study including patients treated with a GLP-1RA together with a sodium glucose transporter 2 inhibitor (SGLT2), the mean reduction of glucose was 2.2 mmol/L (39.6 mg/dL) (p < 0.0004) after 6 months [17]. This therapeutic combination achieved not only adequate glycaemic control, but also weight loss (2.1 kg; p < 0.00003) and decrease of blood pressure [17]. In addition, 34.3% of patients achieved Hb1Ac levels <7% and weight loss >5%, without hypoglycaemias [17]. These results are also supported by another real-world observational study in with patients receiving a GLP-1RA in combination with metformin and a SGLT-2 inhibitor [18].
The main adverse effects of GLP-1RAs are gastrointestinal: nausea, vomiting, diarrhoea and abdominal complaints (see Table 2) [19]. However, these are mostly self-limited over time [19]. Another adverse effect is injection-site reactions [19]. Moreover, there are indications that incretin-based therapies may cause pancreatic diseases. Nevertheless, according to real-world evidence, the risk of pancreatic disease associated with add-on GLP-1RAs to metformin therapy appears to be no higher than that associated with other antidiabetic agents [20].
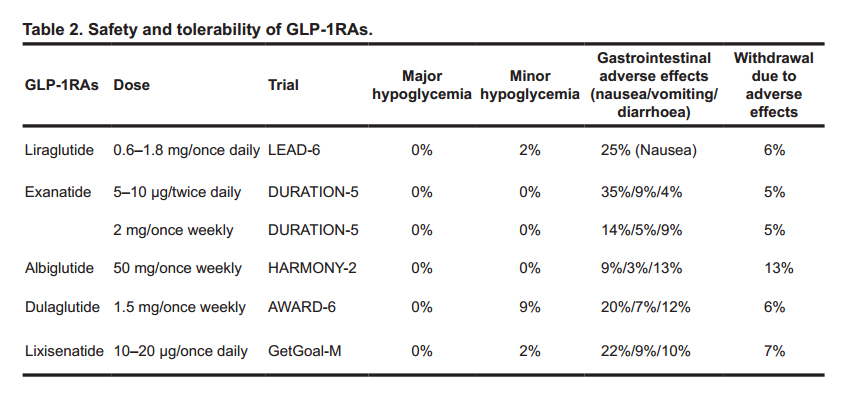 Table 2. Safety and tolerability of GLP-1RAs.
Table 2. Safety and tolerability of GLP-1RAs.
Obviously, the need for injection may discourage some patients, but this can easily be overcome with patient education [16,19]. Moreover, the new pens and (especially) the once-weekly injection of some compounds render them more user friendly [11,16,19]. Another consideration is administration and ease of use. For example, albiglutide needs reconstruction before injection, making its use difficult for some patients, including those with visual or dexterity issues [11,16,19].
The most important challenge for GLP-1RAs is, as indeed for all antidiabetic agents, the potential cardioprotective actions [21,22]. In this context, GLP-1RAs have demonstrated: (a) slight improvements in arterial pressure, lipid parameters and inflammation in humans; (b) improvements in heart failure and myocardial infarction in the experimental setting [21–24].
Of particular relevance, GLP-1RAs exhibit important differences in their cardiovascular effects in large clinical trials. Indeed, liraglutide and semaglutide significantly reduce the risk of major adverse cardiac events [25,26]. By contrast, once-weekly exenatide and lixisenatide have shown a neutral cardiovascular effect: safety but no benefit [27,28]. These differences need to be appreciated in clinical practice, especially when prescribing antidiabetic treatment to patients with known cardiovascular morbidity [29,30].
Importantly, in the most recent cardiovascular outcomes trial [31], once-weekly albiglutide reduced the primary cardiovascular endpoint by 22%, exhibiting superiority compared with placebo (p = 0.0006). This trial further enhances the importance of GLP-1RAs, especially in patients with established cardiovascular disease [31,32].
Furthermore, there is recent evidence that that GLP-1RAs may improve the natural history of diabetic complications. A pharmacovigilance meta-analysis has demonstrated that reduced incidence of retinopathy with GLP-1RAs, as compared to other antidiabetic agents [33]. Importantly, GLP-1RAs appear to exert an additional protective role in the kidneys. According to real-world evidence, their use in patients with low estimated glomerular filtration rate (eGFR) was related to less pronounced reduction in eGFR (−0.80 vs. −1.03 mL/min/1.73 m2, p = 0.0005), as compared with other therapies, while HbA1c was significantly reduced as well [34].
Finally, it is now being increasingly appreciated that GLP-1RAs can be excellently be combined with basal insulin [32]. In this more modern combination, GLP-1RAs target post-prandial hyperglycaemia, while basal insulin targets fasting glucose. Nowadays, fixed GLP-1RAs+basal insulin combinations used as a single daily injection in the same pen are available to increase patient compliance [32].
In conclusion, GLP-1RAs are antidiabetic agents with many advantages [5,8,14,35]. Their beneficial actions are increasingly being appreciated in the treatment of T2DM.
This perspective was written independently. The authors did not receive financial or professional help with the preparation of the manuscript. N. Papanas has been an advisory board member of TrigoCare International, Abbott, AstraZeneca, Elpen, MSD, Novartis, Novo Nordisk, Sanofi-Aventis and Takeda; has participated in sponsored studies by Eli Lilly, MSD, Novo Nordisk, Novartis and Sanofi-Aventis; received honoraria as a speaker for AstraZeneca, Boehringer Ingelheim, Eli Lilly, Elpen, Galenica, MSD, Mylan, Novartis, Novo Nordisk, Pfizer, Sanofi-Aventis, Takeda and Vianex; and attended conferences sponsored by TrigoCare International, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Novartis, Novo Nordisk, Pfizer and Sanofi-Aventis.
N.P. conceived the perspective. T.P. wrote the first draft. N.P. edited and finalised the manuscript.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
Penlioglou T, Papanas N. Glucagon-like Receptor 1 Agonists in the Treatment of Type 2 Diabetes. Med One. 2018 Dec 18; 3: e180013. https://doi.org/10.20900/mo.20180013

Copyright © 2020 Hapres Co., Ltd. Privacy Policy | Terms and Conditions




