Location: Home >> Detail
Adv Geriatr Med Res. 2025;7(1):e250004. https://doi.org/10.20900/agmr20250004
 ,
Michael Kehrer 1 ,
Dieter Christian Wirtz 1 ,
Hendrik Kohlhof 2,*
,
Michael Kehrer 1 ,
Dieter Christian Wirtz 1 ,
Hendrik Kohlhof 2,*
1 Clinic for Orthopedics and Trauma Surgery, University Bonn, Bonn 53127, Germany
2 St. Antonius Hospital Cologne, Cologne 50968, Germany
* Correspondence: Hendrik Kohlhof.
Demographic change, accompanied by its complex requirements, represents a major challenge for today’s orthopedics and traumatology departments. The “geriatric patient”, is moving into focus, and increasingly requires geriatric-internal co-treatment in addition to orthopedic-injury surgery expertise.
This retrospective case–control study investigated how the co-treatment by a geriatrician in orthopedic patients influences drug prescriptions, and whether and how an improvement in drug safety and more adequate pharmacotherapy can be achieved. The FORTA list established for the German-speaking region was used as the evaluation standard. Therefore, FORTA AB resulted from the total sum of the respective admissions or discharge medications, minus the FORTA-C and D hits. For the study, the FORTA categories C and D listed medications were considered particularly relevant because they are high-risk, and they were statistically reviewed during the study. A total of 54 patients in the study group (GOKM group) were treated according to the integrated geriatric orthopedic concept, compared to 59 patients in the reference group (OM group). In order to precisely test for an analysis of variance was performed with a mixed-design analysis of variance (ANOVA).
ACE, angiotensin converting enzyme; ADRs, adverse drug reactions; ANOVA, analysis of variance; ASA, acetylsalicylic acid; ATC, anatomical therapeutic chemical; ATZ, geriatric trauma centers; DGG, German Society for Geriatrics; DVT, deep venous thrombosis; ESC, European Society of Cardiology; EUGMS, The European Union Geriatric Medicine Society; FORTA, Fit for the Aged; GCT, geriatric complex treatment; GDS, Geriatric Depression Scale; GOKM, geriatric-orthopedic co-management model; HDL, high-density lipoproteins; HIT, heparin-induced thrombocytopenia; HTI, hip TEP infections; ICU, intensive care unit; KTI, knee TEP infections; LMWH, low-molecular-weight heparin; MMSE, Mini-Mental State Examination; n-PIM, not potentially inadequate medication; NSAIDs, nonsteroidal anti-inflammatory drugs; OM, orthopedic management; PAO, periarticular ossification; PIM, potentially inadequate medications; PTCA, after percutaneous transluminal coronary angioplasty; PTT, partial thromboplastin time; TEP, total endoprosthesis; TIA, transient ischemic attack; TUG, Timed Up & Go; UFH, unfractionated heparin
Demographic change, accompanied by its complex requirements, represents a major challenge for today’s orthopedics and traumatology departments. In 1991, the number of people >65 years of age in Germany was 12 million (15% of the total population); in 2019, this figure has already increased to 18 million (22% of the total population). The number of people >80 years of age in Germany almost doubled during this period, and now comprises around 2.4 million people. The Federal Statistical Office expects this population group to grow to more than 10 million people by the year 2050 [1]. One potential consequence of patient complexity is insufficient peripheral care, which is also reflected in diagnostics and therapy. For example, Steinmann et al. showed that two-thirds of polypharmaceutically-treated patients were inadequately medicated [2].
The “geriatric patient” is defined as follows: older than 65 years but more likely 70+, multimorbid, and on polypharmaceutical drug treatment, is moving into focus, and increasingly requires geriatric-internal co-treatment in addition to orthopedic-injury surgery expertise. The average woman over 80 years of age comes with about 3.6 pre-existing conditions/diagnoses, and men of the same age have 3.2 diagnoses [3], which usually require drug treatment [4].
Polypharmacy, a term which is not uniformly defined but is usually specified as more than five prescribed medications, harbors considerable potential for complications [5,6]. The reasons for this are altered tolerability and metabolism compared to young people, but also problems of adherence due to e.g., cognitive decline in dementia syndromes [7,8]. In this study, taking five or more drugs daily was classified as polypharmacy.
With each drug, the potential risk of possible adverse drug reactions increases, as well as drug interactions that may result in patient harm or deterioration of the surgical outcome. A 2020 U.S. study found that 44% of men and 57% of women use five or more different drugs daily, and 10% exceed the critical threshold of more than 10 different substances [9,10]. Adverse drug reactions (ADRs) are estimated to be the cause of 6.5% of all hospital admissions through the emergency department [11]. The resulting deaths can only be estimated inaccurately, but numbers between 16,000–40,000 deaths per year are suspected [12]. In addition, according to a British study, around 700 million euros in additional costs per year and a constant capacity commitment of 5600 beds are associated with this problem [13].
Multimorbidity refers to the simultaneous presence of several, usually chronic, diseases in one patient [14]. This often results in polypharmaceutical treatment or multimedication [15], social withdrawal, and loneliness [16], which finally leads to an increased risk of mortality [17]. Since 2015, the university presence of geriatrics has expanded from 6 to 16 of the 37 medical faculties [18].
In 2017, the Clinic for Orthopedics and Traumatology at Bonn University Hospital initiated the project of geriatric orthopedic integrated care in cooperation with the geriatric department of Malteser Hospital Bonn. Similar to the concept of the geriatric trauma centers (ATZ), an attempt is now being made to offer orthopedic patients, who often undergo elective surgery, improved perioperative care, as well as an early rehabilitative concept. For this purpose, patients are included in geriatric complex treatment (GCT), with a minimum length of hospital stay of 16 days and 20 therapy sessions performed by the accompanying physiotherapists and occupational therapists. In this study, the interaction between geriatricians and orthopedic surgeons is referred to as the geriatric-orthopedic co-management model (GOKM).
Hypothesis, Research Question, and ObjectivesThe purpose of this study was to investigate the effect of co-treatment with a geriatrician in orthopedic patients on medication prescriptions, and whether and how this could be used to improve drug safety and thus encourage more adequate pharmacotherapy. Furthermore, the insufficient peripheral care of geriatric patients was also addressed. The aim of the study was to prove that care by a geriatrician primarily causes an objectifiable optimization of the medication schedule of multimorbid and polypharmaceutically treated patients in the pre- and perioperative process, which secondarily has a positive effect on the postoperative outcome. The evaluation standard for drug safety in geriatric patients was that used for the FORTA list.
1.
2.
3.
4.
5.
The literature search was performed manually via Medline, by means of Pubmed (National Center for Biotechnology Information), as well as automatically via the search function of the literature management program Citavi 6 (Version 6.8—Free on https://www.citavi.com/download). In addition, Google Scholar was used as a database [19].
Lists of Potentially Inadequate Drug Agents in the ElderlyThe PRISCUS list and FORTA list are tools for monitoring and changing drug treatments in geriatric patients in German-speaking countries. The first version of such a list was the Beers List in 1991, which was created by the U.S. geriatrician Mark H. Beers. Beers was the first to list potentially inadequate medications (PIM) that were not recommended for treating the elderly. In 1997, 2003, and 2012, the Beers list was revised and updated several times, but at its core remained a negative list that did not specify “explicit criteria” for why a particular agent is potentially inadequate and what alternative treatment options are available [20]. Because there was no evidence to support the applicability of such a medication list, its clinical benefit was questionable [21].
The PRISCUS list was created in 2010 by pharmacologist Petra A. Thürmann as an adaptation of the Beers list to the drug specifics and the market situation in Germany [22,23], including drugs that have an increased risk-benefit profile, particularly in geriatric patients. A Likert scale was used (1 inadequate = PIM, 5 potentially safe = n-PIM). A total of 83 drugs were listed as PIM and 26 as not potentially inadequate medication (n-PIM), and 46 active ingredients could not be clearly assigned by expert panels even after two rounds of analysis [20,22]. With more than 100 active substances, this list represents only a fraction of the available and applied drugs. For this reason, after data collection for this study, it was decided not to include an analysis of this data.
The FORTA concept of Professor Dr. Med. Peter Wehling and the resulting list was a further development made by the University of Heidelberg and the Medical Faculty of Mannheim of the abovementioned “negative lists” [24]. FORTA is an acronym and stands for “Fit for the Aged”. The list was last revised in 2019 and includes approximately 290 active drug substances, which are divided into categories A–D. Here, drugs with a clearly positive risk-benefit profile were classified in group A, as “absolutely” recommended. These include, for example, antihypertensives such as angiotensin converting enzyme (ACE) inhibitors for arterial hypertension or diuretics for heart insufficiency. Substances with a proven benefit but potential for ADRs, such as beta-blockers, were assigned to category B. Potentially adverse benefit-risk profiled substances were assigned to group C, including e.g., amiodarone in heart failure. Absolutely inadequate substances were classified in category D, such as nonsteroidal anti-inflammatory drugs (NSAIDs) in the form of ibuprofen in long-term pain treatment, or benzodiazepines for the treatment of agitation.
The categorization depends on the indication, e.g., an active substance can be assigned to category A, B, or C depending on the indication. An example is the prescription of diuretics, depending on the indication and the associated classification. In the case of cardiac insufficiency, this is considered to be absolutely recommended (category A), but if there is arterial hypertension that is difficult to control, the diuretic is assigned to category B.
Thus, the FORTA list can be used as a decision support tool for complex pharmacotherapies of multimorbid geriatric patients, and provides alternatives that the user can apply to the individual [25–28]. In this work, the 2015 version of the FORTA list was used as the basis for reviewing medication lists.
Study DesignThis was a retrospective case–control study. The treatment focus was primary arthroplasty and revision arthroplasty in multimorbid geriatric patients. The study sample included patients treated in the first year of the geriatric-orthopedic concept and is characterized as the GOKM group. The reference group did not receive geriatric co-management and was designated as orthopedic management (OM). Data collection was from the electronic patient file (admission record, emergency record, discharge summary). Parameters collected were age, length of hospital stay, gender, main diagnosis, surgery, revision, delirium/dementia, number of A-medication and E-medication, FORTA hits. Here, the drugs listed in the FORTA list in categories C and D were considered relevant for the study.
Patient CohortThe study population consisted of 113 patients with an International Statistical Classification of Diseases and Related Health Problems (ICD) coded 84.x principal diagnosis who were undergoing treatment predominantly for primary arthroplasty or revision arthroplasty. At the time of treatment, the patient had to be older than 70 years, have multimorbid disease, and be treated with polypharmacy. A total of 54 patients in the study group (GOKM group) were treated according to the integrated geriatric orthopedic concept from 1 April 2017 to 31 December 2017, compared to 59 patients in the reference group (OM group), which were enrolled from 1 January 2016 to 4 January 2017 (Supplementary Table S1).
Data CollectionAfter initiation of the geriatric orthopedic concept, a list of all patients who were discharged according to OPS 8-550 (early complex geriatric rehabilitation therapy) was compiled. One year after completion of therapy, this list was used as the basis for the study group. Using the patient information, the corresponding virtual patient record could be consulted, and the necessary diagnoses, surgeries, medication plans, and epicrisis could be analyzed.
The total of all prescribed admissions, as well as discharge medications, of each patient was recorded. The drugs noted in the FORTA list were then manually compared with the patients’ medication plans. If a hit was found in the analysis, these drugs were included in a Microsoft Excel database.
Subsequently, the indication was checked based on the known diagnoses and, in case of doubt, after inspection of the epicrisis and, thus, classification as A, B, C, or FORTA D. Hits in the FORTA-A and B categories were combined and not nominally included in the database. Therefore, FORTA AB resulted from the total sum of the respective admissions or discharge medications, minus the FORTA-C and D hits. For the study, the FORTA categories C and D listed medications were considered particularly relevant because they are high-risk, and they were statistically reviewed during the study.
For the reference group, a manual patient selection was performed in the hospital information system (HIS) Orbis version 08043702. 01000.DACHL. The inclusion criteria for recruitment were a date of birth between 1 January 1920 and 12 December 1943, length of hospital stay from admission day 1 January 2016 to 4 January 2017, and principal diagnosis ICD T84. Patients who died during their stay or who were not given any surgical therapies were excluded. If discrepant diagnoses were found in the search of patients’ records, including the epicrisis, in the physician’s letter, the patients were also excluded.
Data PreparationAn Excel table was created with the complete data sets, which contained all relevant patient information. From this, tables of population characteristics, diagnoses and operations, medications, and hits were extracted for further statistical processing and exported to SPSS version 27. For a possible substance group classification, internationally valid Anatomical Therapeutic Chemical (ATC) codes were assigned to the prescribed drugs.
Statistical Evaluation and Descriptive Data AnalysisAll statistical analysis was performed using the software programs Microsoft Excel (version 2208 USA) and SPSS for Windows (version IBM 23.0 USA). Drug-related and person-related statistical analysis was performed.
In the descriptive analysis, absolute and relative frequencies, median, arithmetic mean, and standard deviation are shown. Bar charts were created for visualization.
Advanced Statistical Significance TestingStudent’s t-test for unpaired samples was used to test for significant differences between two subgroups of the patient population. It was considered significant if p < 0.05 (with p < 0.01 indicating highly significant).
To test the independence of a dichotomous characteristic in independent samples, Fisher’s exact test was used. The same significance levels applied as for the t-test.
The chi-square test, also known as the distribution test, checks data for stochastic independence and/or whether multiple samples are homogeneously distributed.
The Mann–Whitney U test was used to test the significance of non-parametric correlations. For non-normally distributed variables, the U-test and Wilcoxon rank sum test were used for investigation.
Prescription Tendency or Individual Drug AnalysisThe prescription trend was determined manually using an auxiliary table. Here, the trend of prescribed drugs on admission was determined in comparison to the number of prescriptions on discharge. If there were four prescriptions on admission and five on discharge, for example, this was considered an increase. The amount of the difference was not taken into account. For example, if there were nine prescriptions on admission and two on discharge, this was considered a reduction. A scaling into e.g., strong reduction etc. did not take place.
Finally, in order to precisely test for an influence of e.g., a strong reduction or a strong tendency toward new prescriptions, an analysis of variance was performed with a mixed-design analysis of variance (ANOVA), including the within-subject variables (FORTA-C and D). Because of the two different measurement times, the variables contained two levels each (FORTA-Hits admission and discharge). The between-subject variables were group classification OM and GOKM. This was considered significant if p < 0.05 (p < 0.01 highly significant).
Comparison of the population characteristics shows that there were no significant differences in gender, age, or septic surgeries performed. Differences were seen in the length of stay and the number of revisions (Table 1). The GOKM group had 16 patients with significantly more revisions than the OM group. This was also true for the length of hospital stay, which, as expected, was significantly longer due to GCT. There were no data for the possible presence of dementia or the occurrence of delirium in the OM group. In the GOKM group, the diagnosis of delirium was made a total of 12 times, with seven of those diagnoses being confirmed. With regards to the presence of dementia, there were 10 suspected cases, with two diagnoses confirmed. GCT was completed in 37 cases. For the terminated cases, either the therapy units were not available for fulfillment, an unscheduled transfer/surgery occurred, or the minimum length of stay was not achieved (Supplementary Table S2, S3, S4, S5) (Supplementary Figure S1).
 Table 1. Population characteristics.
Table 1. Population characteristics.
In terms of coded stay diagnoses, there was a statistically significant difference between the two groups regarding hip total endoprosthesis (TEP) infections (HTI) and knee TEP infections (KTI), septic hip TEP loosening, and native knee joint infections (Figure 1).
In the individual analysis, with p = 0.01 in the Fisher’s exact test, there were significantly more HTI and native knee joint infections in the GOKM compared to the OM group, but more KTI and septic hip TEP loosening in the OM group.
Consistent with the diagnoses, the statistics for surgeries performed with Fisher’s exact test (p = 0.01) revealed a statistically significant difference in hip and knee TEP implantations (Figure 2). More hip TEP implantations were performed in the GOKM group, whereas more knee TEPs were performed in the OM group. Regarding the performed implantations, there was a homogeneous distribution without significant differences. (Supplementary Table S5, S6, S7, S8).
 Figure 1. Coded diagnoses. Note: * indicates statistically significant; p = 0.01 by Fisher’s exact test; significantly more hip TEP infections and native knee joint infections in the GOKM group vs. more knee TEP infections and septic hip TEP loosening in the OM group.
Figure 1. Coded diagnoses. Note: * indicates statistically significant; p = 0.01 by Fisher’s exact test; significantly more hip TEP infections and native knee joint infections in the GOKM group vs. more knee TEP infections and septic hip TEP loosening in the OM group.
 Figure 2. Statistics of performed surgeries. Note: *statistically significant differences; p = 0.01 Fisher’s exact test; homogeneous distribution for performed implantations without significant differences; significant difference with statistical significance regarding hip and knee TEP implantations.
Figure 2. Statistics of performed surgeries. Note: *statistically significant differences; p = 0.01 Fisher’s exact test; homogeneous distribution for performed implantations without significant differences; significant difference with statistical significance regarding hip and knee TEP implantations.
The descriptive statistics of the total medication at hospital admission showed that a median of 10 preparations were prescribed in the GOKM group, compared to nine in the OM group (Table 2). A range from a minimum of one to a maximum of 21 different drugs was detected in the GOKM group (0 to 18 drugs in the OM group). Further statistical analysis using the Mann–Whitney U test did not reveal any statistically significant differences. This was not the case for the total medication at discharge. With a median of 14 active substances, there were significantly more prescriptions in the GOKM group than in the OM group, with a median of 11 prescriptions (Mann–Whitney U test p = 0.002). The min–max range revealed no drug-naive patients in the OM group (4 to 21 prescriptions). The maximum of different preparations also slightly increased in both groups, with 23 (GOKM) and 21 (OM), respectively.
Analysis of the descriptive statistics by classification into FORTA A+B, FORTA-C, and FORTA-D at admission showed that more prescriptions of A + B, as well as C-hits, were recorded in the GOKM group compared to the OM group, but slightly fewer D-hits. However, a statistically significant difference was found only for FORTA-C (p = 0.01). Thus, 420 and 449 AB-hits, 42 and 62 C-hits, and 50 and 42 D-hits were present at admission from the perspective of the GOKM group. This was due to the patient groups which had already recorded two and three hits at admission.
Evaluation of the discharge medication showed, as at admission, that there was a significant difference in the FORTA-C medications (p = 0.012). Thus, 54 prescriptions could be detected in the OM group and 86 FORTA-C prescriptions for the GOKM grouping. An absolute increase in prescriptions in both groups was also shown for FORTA A+B. However, with 506 hits in the OM group to 572 hits in the GOKM group, there was no statistical relevance in the Fisher’s exact test (p = 0.476). FORTA-D hits were only slightly different, with 55 in the OM group to 52 hits in the GOKM group (p = 0.728).
 Table 2. Descriptive statistics and significance testing of medication.
Table 2. Descriptive statistics and significance testing of medication.
With regards to prescribing behavior, it was found that the majority of patients increased their total medication during the treatment period. In the GOKM group, 68.5% of patients had at least one new prescription after completion of complex treatment, and in the OM group 81.4% of patients had the same (Figure 3).
There was no statistically significant reduction in total medication. Although the GOKM group tended to reduce total medication in 14.8% of cases, the OM group reduced it in only 3.4% of cases. However, this was not statistically relevant (Fisher’s exact test p = 0.10).
 Figure 3. Prescription trend of the total medication. Note: The prescription trend for total medication generally showed an increase in medication in both groups. Increased reductions occurred in the GOKM group, but this difference was not statistically significant. Fisher test p = 0.1.
Figure 3. Prescription trend of the total medication. Note: The prescription trend for total medication generally showed an increase in medication in both groups. Increased reductions occurred in the GOKM group, but this difference was not statistically significant. Fisher test p = 0.1.
Examination of this characteristic revealed that there was an increase in prescriptions in 38.9% of the GOKM patients and in 25.4% of the OM group (Figure 4). A reduction occurred in three cases each, corresponding to 5.6% and 5.1%, respectively. The Fisher’s exact test, however, showed no statistical significance (p = 0.31) (Supplementary Figure S2, S3).
 Figure 4. Prescription trends of drugs with FORTA-C listing. Note: data in %; Fisher’s exact test showed no statistically significant differences (p = 0.31).
Figure 4. Prescription trends of drugs with FORTA-C listing. Note: data in %; Fisher’s exact test showed no statistically significant differences (p = 0.31).
FORTA D, a drug group considered potentially high-risk, saw an increase in hits in more than twice as many patients (27.8%) in the GOKM group, compared with 13.6% in the OM group. Hit-reduction occurred in 11.9% of the OM group and 14.8% of the GOKM group. However, the absolute values did not prove to be statistically significant (Fisher’s exact test, p = 0.11) (Figure 5) (Supplementary Figure S4, S5).
 Figure 5. Prescription trends of drugs with FORTA-D listing data in %. Note: Fisher’s exact test showed no statistically significant differences (p = 0.11).
Figure 5. Prescription trends of drugs with FORTA-D listing data in %. Note: Fisher’s exact test showed no statistically significant differences (p = 0.11).
1.
2.
3.
In total, 132 hits were observed in the study population, consisting of 86 FORTA-C hits and 52 FORTA-D hits. A total of 102 of these negative hits were explicable when looking at the indication and the guidelines. A total of 22 FORTA-C hits were due to the prescription of low-molecular-weight heparin (LMWH) and unfractionated heparin (UFH) in the context of prolonged bridging. Another 32 mixed hits were due to seven neuroleptics, ten anticonvulsants, and 15 antidepressants in the context of analgesic therapy for mixed pain, depression due to chronic pain, and delirium. Seven FORTA-D hits were caused by the prescription of acetylsalicylic acid (ASA) 100 mg without any indication, which will be discussed further in a later section. Another 15 FORTA-C hits were due to opioid analgesics (tilidine/naloxone = 11; fentanyl = 1; oxycodone/naloxone = 3) in the context of the World Health Organization (WHO) analgesic ladder. The 26 FORTA-D hits can be explained in the same context. Thus, a total of 20 ibuprofen, 3 diclofenac, and 6 coxibes were prescribed. The former has the benefit of prophylaxis after orthopedic surgery (PAO) in addition to the analgesic component. Overall, the use of ibuprofen was reduced from approximately 51% in the reference group to 37% in the intervention group (Supplementary Table S9).
Results on Insufficient Care, Analgesia, and Delirium ManagementWith regards to the assumed lack of ambulatory care, the GOKM group showed that the criteria for polypharmacy were fulfilled, with a median of 10 different medications on admission. As expected, further prescriptions were issued in the course up to discharge, so that a median of 14 different preparations were found in the medication plans at discharge. An increase of 40% more prescriptions compared to the time of admission at the time of discharge seems to support the hypothesis at first glance, but this must be put into context when taking a closer look at the cohort studied. Patients undergoing revision arthroplasty usually require antibiotic follow-up and are rarely discharged with fewer analgesics than at the time of admission. From this perspective, based on absolute numbers, and also on the basis of FORTA hits, there was no peripheral underuse.
Analgesic therapy was changed in the study group to the extent that approximately 50% fewer ibuprofen prescriptions were noted at discharge (Figure 6). Thus, GOKM showed a statistically significant reduction of ibuprofen, with an increased tendency to prescribe WHO level 2 analgesics and hydromorphone, a substance classified as FORTA-B. Pregabalin was also prescribed four times, especially in cases of mixed pain.
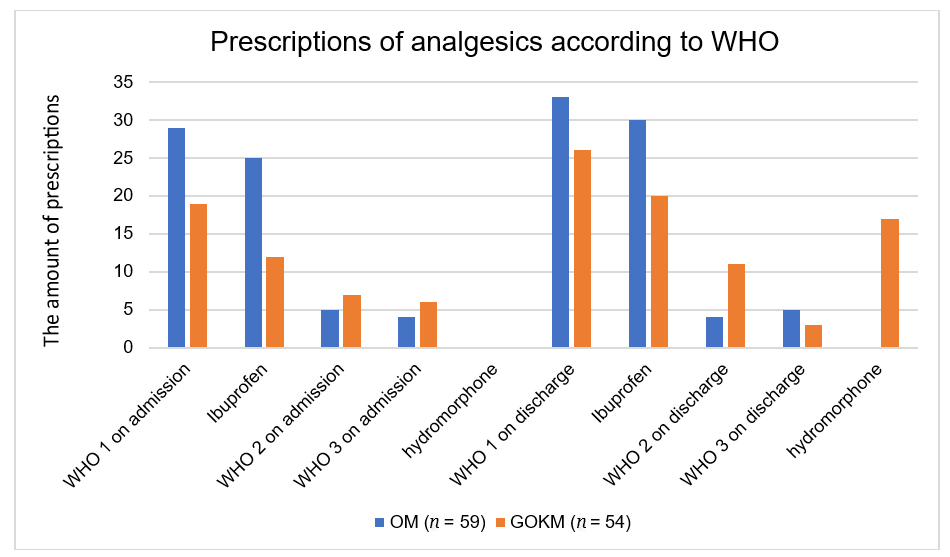 Figure 6. Prescriptions of analgesics according to WHO. Note: WHO 1 consisting of ibuprofen, coxibes, diclofenac; WHO 2 consisting of tilidine/naloxone and tramadol; WHO 3 consisting of morphine, fentanyl, and oxycodone. Hydromorphone recorded separately due to FORTA-B classification.
Figure 6. Prescriptions of analgesics according to WHO. Note: WHO 1 consisting of ibuprofen, coxibes, diclofenac; WHO 2 consisting of tilidine/naloxone and tramadol; WHO 3 consisting of morphine, fentanyl, and oxycodone. Hydromorphone recorded separately due to FORTA-B classification.
A positive influence of the geriatricians in the GOKM group was shown with regards to the group of neuroleptics used off-label for the treatment of delirium (Figure 7). Looking at the continued and new prescriptions, as well as the discontinuation of any substances, two continued prescriptions were made in the OM group, while in the study population there were three continued prescriptions and four new prescriptions. Twice, substances of this group were discontinued. These dynamics show that the 12 delirium states diagnosed in the study population were adequately treated pharmaceutically.
 Figure 7. Prescribing trends of neuroleptics in off-label use for delirium visualization of prescribing dynamics in GOKM and prescribing inertia in OM.
Figure 7. Prescribing trends of neuroleptics in off-label use for delirium visualization of prescribing dynamics in GOKM and prescribing inertia in OM.
Similar results were obtained in the use of antidepressants (Figure 8). In the GOKM group, four patients were classified as depressed and initiated antidepressant therapy. Assuming the same prevalence, the number of undiagnosed and untreated depressions in the OM group can be assumed to be around 27%.
 Figure 8. Prescriptions of antidepressants.
Figure 8. Prescriptions of antidepressants.
The aim of this study was to examine the concept of geriatric-internal medicine complex treatment in terms of its outcome with regards to drug safety. The GOKM group showed a prolonged length of hospital stay compared to the OM group, which can be explained by the scheduled longer care within the GCT. Comparison of the surgeries performed showed an increased number of hip TEP explantations in the GOKM group, which was associated with the increased diagnosis of hip TEP infection in this group. This was also evident in the OM group, in which the number of knee TEP explantations was associated with concomitant increased knee TEP infections compared to the GOKM group. Overall, there were more revision surgeries in the GOKM group compared to the control group. This may be due to several reasons.
First, it is necessary to distinguish between hip TEP infections and septic hip TEP loosening, because highly florid infections of the hip in perioperative management are not comparable to a low-grade infection of the inserted prosthesis, which can lead to septic hip TEP loosening. Furthermore, it is important to know that patients who have already undergone a revision due to a periprosthetic infection have an increased risk of revision compared to patients who have not undergone a revision [29–31]. The Endoprostheses Register Germany indicates a probability of up to 40% for a new revision procedure within three years after the first replacement, provided that the indication for the first replacement was a periprosthetic infection [32]. In the context of our study, it can be concluded that there were 17 patients in the GOKM group who had already been revised at least once in the surgical area, and thus had an increased risk of revision compared to the OM group, in which only 12 patients had been previously revised in the surgical area in question. The statistically significant difference in diagnoses and surgeries performed between the GOKM and OM groups should therefore be seen as a limitation of this study. To achieve better comparability in future studies, the diagnoses and surgeries performed in the GOKM, and OM groups should be equally distributed, in addition to the already adjusted population characteristics, to obtain the best matched patient population.
Regarding drug safety and medication quality, our study did not show any significant difference measurable by the FORTA list in GOKM patients compared to OM patients from admission to discharge (ANOVA). The hypothesis that there would be an overall increase in total medication and prescriptions was confirmed. However, the hypothesis that co-management would result in a reduction in high-risk stratified FORTA C and D prescriptions was refuted. This can be explained by the fact that the investigated patient cohorts already required a large number of medications for antihypertensive and antidiabetic therapy, for example, due to multimorbidity, and the investigated patients required additional medication postoperatively for pain reduction and thrombosis. The non-measurable success and quality improvement of co-management only becomes apparent when the underlying indications of the prescriptions made are examined. Reference was made to this in Section 4.2 “Reasonable hits in the study population”. Whether the interaction of the geriatricians led to a reduction of ADRs cannot be proven with the collected data and is therefore hypothetical. In this setting, and especially in polypharmaceutically treated geriatric patients, ADRs are frequent, with 2.4 cases per 100 patients treated, but a direct assignment of the triggering substance is often not possible [33]. This is due to the fact that, for example, in the case of underlying renal insufficiency, an active substance or metabolite must first accumulate in order to trigger problems. This is the case, for example, with deep venous thrombosis (DVT) prophylaxis with LMWH, which can lead to bleeding problems in connection with chronic renal insufficiency.
Matched to this, a statistically significantly increased number of C-hits according to the FORTA list was shown in the GOKM group at discharge (p = 0.01) and admission (p = 0.012). There was no statistically significantly higher reduction in FORTA C and FORTA D hits in the GOKM group; on the contrary, there was even a greater increase in FORTA hits. At first sight, this seems to be a contradiction to the claim of better patient safety due to geriatric-orthopedic cooperation, but on closer examination the opposite was true. Although the FORTA list can be used to assess patient and medication safety in geriatric patients, the type of medication is not the exclusive determinant of patient outcome. Rather, there is a complex interaction of multiple factors. Crucially, delirium predictors such as anemia and pain also have an influence on the postoperative outcome [34–36]. Furthermore, studies also show a clear positive influence through improved mobilization and training of cognitive abilities [37], which enables the GCT performed in the GOKM group to a significantly improved extent. As a result, opioids were also prescribed for improved delirium prophylaxis, which, although considered a hit, can be classified as less serious in the context of geriatric-internal medicine cooperation than the risk of suffering delirium due to severe postoperative pain. The fact that unrecognized or untreated delirium is associated with increased mortality [38] also led to a corresponding increase in prophylactic medication by geriatricians. For example, the S3 guideline for Analgesia, Sedation, and Delirium Management in intensive care medicine recommends analgesia with opioid analgesics for severe pain, even in elderly patients [39]. The consensus among the different studies here is that as much as necessary but as little as possible should be prescribed [40]. In addition, a paradigm shift has taken place that no longer declares polypharmacy to be poor per se. In line with our results, comparable studies have shown that the amount of medication prescribed with geriatric co-treatment increases [41]. However, it is this outside expertise, which puts the focus of attention on the internal complications and underlying diseases, that significantly improves patient safety in the geriatric-orthopedic concept [42]. A suitable measurement instrument for this could be, for example, newly diagnosed secondary diagnoses, such as cardiac decompensation or nosocomial pneumonia, which were successfully treated with medication.
Reasonable Hits in the Study Population Discussion on bridging new oral anticoagulants (NOAC) with LMWH and UFHIn this study, prolonged bridging was demonstrated for 22 of 54 patients (40.7%), which at first glance seems inadequate. In postoperative courses with few complications, such as primary hip TEP implantation in an average patient, rapid resumption of oral anticoagulation in the hospital setting would be the best possible therapeutic option. However, the rather high number of revision patients puts this fact into context and may explain prolonged bridging. Furthermore, there is no solid data on when it is optimal to restart therapy with NOACs. Factors such as individual patient bleeding or thromboembolism risks, surgical method and length, blood loss, and mobility all play a role [43]. In this regard, the blanket statement (Forta-HIT-C in bridging) should be considered highly critical. LMWH in therapeutic doses are prescribed for the standard procedure [25]. Bridging by using high LMWHs/UFHs must be considered problematic, as these are administered by means of syringe pump under regular partial thromboplastin time (PTT) control. Time and manageability, as well as different response and heparin-induced thrombocytopenia (HIT) 2 risk to the drug, often leads to overtreatment or PTT in the non-therapeutic range. However, in individual cases of e.g., artificial heart valves or terminal renal failure, exactly this type of bridging is absolutely correct [43]. Based on the study population and the increased number of revisions, clinically the use of heparins can be considered beneficial with regards to bleeding complications in such emergency surgeries. However, the optimization of in-hospital logarithms according to risk stratification B postulated in the FORTA list is not possible in this context. For future studies, the hypothesis of a lower transfusion probability would have to be postulated and investigated.
LMWH: This substance group registered on the FORTA list. For this study, LMWHs with this indication and an administration time longer than 14 days were classified as FORTA-C. A final evaluation, consultation, and approval by Prof. Wehling were conducted.
Argumentation for the use of ASA 100In the experimental group, the use of ASA 100 was documented a total of seven times without a clear indication or atrial fibrillation recorded as a previous cardiological condition. Secondary prophylaxis with ASA after percutaneous transluminal coronary angioplasty (PTCA) and stent implantation after apoplexy with transient ischemic attack (TIA) or vascular surgery is undisputed, and also mentioned by the guidelines of several medical societies (e.g., the European Society of Cardiology (ESC)).
For a long time, the use of ASA in primary prophylaxis of cardiogenic disease has been controversial, as the ARRIVE-Study (A Randomized Trial of Induction Versus Expectant Management) and A Study of Cardiovascular Events in Diabetes (ASCEND) trials most recently showed only marginal benefit versus increased risk of bleeding [44,45]. Thus, the current ESC guideline does not recommend the use of low-dose ASA in patients without cardiovascular disease [46]. The situation is different in the presence of any cardiovascular risk factors, such as dyslipidemia, arterial hypertension, diabetes mellitus, or evidence of vascular damage. Here, the guidelines advocate an individual therapy decision depending on the cardiovascular risk score, based on age, total cholesterol, high-density lipoproteins (HDL), nicotine consumption, and systolic blood pressure level, with a recommendation grade of III/B to IIb/A [47]. Knowing that the origin of atrial fibrillation is due to vascular changes in the heart caused by macro- and micro-angiopathies in about 30% of cases, and another 30% are due to structural cardiac changes, such as valvular abnormalities or hypertrophy of the myocardium, it can be assumed in relation to the experimental group that the prescription of ASA was justified.
Argumentation for the use of neuroleptics in delirium managementThe German S3 guideline on “Analgesia, Sedation and Delirium Management in Intensive Care Medicine” describes “some evidence” for neuroleptics, alpha-2 agonists, and benzodiazepines for the treatment of delirium. The latter, in particular, are classified as potentially high-risk by the FORTA list, which is in sharp contrast to the guidelines [48]. The best possible risk stratification for the available substances is FORTA C. However, the recommendations were not written specifically for the treatment of elderly patients, but also for children, polytrauma patients, and pregnant and lactating women. The German Society of Geriatrics has also not issued any explicit guidelines for the treatment of delirium, so the use of neuroleptics must currently be described as “off-label use”. The scientific data are limited. There is evidence of a positive effect of neuroleptics in delirium therapy, although the “low level of evidence” in the existing studies must be taken into account [49].
Applied to the delirium management in the GOKM group, this means that any intervention meant a potentially dangerous treatment according to FORTA, but the patient could/did clinically benefit from this, because a potentially life-threatening brain-organic condition was adequately treated [50].
Another positive aspect shown in the study is that the clinical entity delirium was diagnosed. Hypoactive delirium is especially underdiagnosed, but in the perioperative setting mixed type delirium is also difficult to diagnose, because potential symptoms like restlessness, confusion, fatigue, and attention deficit could be triggered after anesthesia or by pain [25]. As far as possible, all conservative measures were applied and possible delirogenic symptoms, e.g., pain, were treated according to the WHO analgesic ladder. As an ultimo ratio, neuroleptics were successfully used to avoid transfer to the intensive care unit (ICU), and further treatment was continued in familiar surroundings and by the multi-professional team known to the patient.
Argumentation for justifiability correction for the use of opioidsThe S3 guideline Analgesia, Sedation, and Delirium Management in Critical Care Medicine recommends analgesia using opioid analgesics for severe pain even in elderly patients [39]. Sufficient pain management may be better achieved with the use of opioid-containing agents compared with high-dose NSAID therapy. This results from the ADRs of NSAIDs, such as renal failure, gastrointestinal bleeding, or even cardiovascular events. Since pain seems to be a strong delirium trigger, sufficient analgesic therapy according to the WHO analgesic ladder is essential to avoid this still underestimated clinical entity, which is associated with a high mortality rate.
Limitations of the StudyRetrospectively, the study design has some limitations, since with regards to the influence to be investigated of geriatric internal medicine expertise, the examination of the visit documentation and the associated prescriptions made during the hospital stay were not recorded.
It is also a weakness that the focus of the study was on potentially dangerous drugs, which could be avoided by intervention, and less on the use of potentially useful drugs. It could also not be excluded that during hospitalization, adjustments in the medication plan could have been made by other specialists, e.g., a neurologist. In the comparison group, the quality of the documentation in the corresponding physician’s letters did not provide a stringent indication for the use of any medication.
In addition, structural limitations in the use of the FORTA lists were found in our study. As in the previously cited study by Wehling, the everyday manageability is rather low due to the time intensity and the complexity of the treated patients. The FORTA list should not be seen as a “negative list” or index for drugs, but as a tool to help find reasonable therapeutic options and alternatives for a specific patient population. Even suboptimal drug treatment is often better than no pharmaceutical intervention. Another structural limitation is that antibiotics are not listed as an “essential” medication. Unlike LMWHs, it was decided not to classify them into categories C or D. Rifampicin, currently the most potent CYP3A4 inducer known to us, enhances the metabolism of opioids, neuroleptics, chemotherapeutic agents, immunosuppressants, antidepressants, calcium channel blockers, macrolide antibiotics, and many other agents. Thus, the aspect of biofilm suppression in implants is a necessary consideration in revision arthroplasty but is achieved by high-risk drug metabolism. It is possible that symptoms such as nausea, confusion, and pain will be triggered, which in turn leads to new prescriptions. Thus, a corresponding adjustment of the medication due to a possible interaction with the antibiotic rifampicin, which is regularly used postoperatively for infections, was not shown.
In conclusion, the hypothesis can be formulated that the examination of patient safety based solely on the prescription numbers of listed medications in the FORTA list is not a sufficient instrument to measure medication safety in geriatric orthopedic patients. Rather, other parameters, such as general condition, delirium frequency, and mobility, should be considered. Due to the lack of data on the frequency of delirium in the control group, this could only be confirmed indirectly in the context of this study. Nevertheless, we continue to believe that optimal adequate patient care should be provided outside of orthopedic expertise by means of geriatric-internal medicine collaborative models. To support this hypothesis, further studies with adjusted study parameters are necessary.
The following supplementary materials are available online at https://doi.org/10.20900/agmr.20250004. Supplementary Table S1: Age distribution in years; Supplementary Table S2: Cohort characteristics according to the patient’s age; Supplementary Table S3: Length of hospital stay in days (d); Supplementary Table S4: Cohort characteristics according to the patient’s hospital stay; Supplementary Table S5: Overview of revision patients; Supplementary Table S6: Cross tabulations: Chi-square tests; Supplementary Table S7: Performed surgeries; Supplementary Table S8: Diagnoses in the OM and GOKM group; Supplementary Table S9: Overview of substances; Supplementary Figure S1: Length of hospital stay; Supplementary Figure S2: Number of FORTA C hits on admission; Supplementary Figure S3: Number of FORTA C-hits at discharge (n); Supplementary Figure S4: Number of FORTA D-hits on admission (n); Supplementary Figure S5: Number of FORTA D-hits at discharge (n).
Ethical review and approval were waived for this study. A retrospective research project exists if, at the time of the question or application, all data to be used have already been collected in full, i.e., they are already available and are thus evaluated purely “retrospectively”. Exclusively retrospective epidemiological research projects are exempt from the obligation to provide advice under § 15 para. 1 BO NW.
Regarding the Informed Consent Statement, informed consent was obtained from all subjects involved in the study. Patients at the University Hospital Bonn sign a privacy policy at the beginning of treatment, as well as a declaration of consent that their collected data may be used anonymously for research purposes.
The dataset of the study is available from the authors upon reasonable request.
Conceptualization, HK and MH; Methodology, HK; Software, MK; Validation, HK, MH, DW; Formal Analysis, MH; Investigation, MH; Resources, MK; Data Curation, MH; Writing—Original Draft Preparation, MH; Writing—Review & Editing, MH; Visualization, MH; Supervision, HK; Project Administration, HK.
The authors declare that they have no conflicts of interest.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
Hoellger M, Kehrer M, Kohlhof H, Wirtz DC. Optimizing Drug Therapy Safety of Geriatric Orthopedic Patients by Providing Integrated Geriatric Care. Adv Geriatr Med Res. 2025;7(1):e250004. https://doi.org/10.20900/agmr20250004

Copyright © Hapres Co., Ltd. Privacy Policy | Terms and Conditions




