Location: Home >> Detail
Adv Geriatr Med Res. 2025;7(3):e250018. https://doi.org/10.20900/agmr20250018
 ,
David Conforti 1 ,
Fatima Tahir 1,* ,
Danielle Ní Chróinín 1,2
,
David Conforti 1 ,
Fatima Tahir 1,* ,
Danielle Ní Chróinín 1,2
1 Department of Geriatric Medicine, Liverpool Hospital, Liverpool, NSW 2170, Australia
2 South Western Sydney Clinical School, UNSW Sydney, Sydney, NSW 2052, Australia
* Correspondence: Fatima Tahir
Purpose: In older people with back pain discharged from hospital, to identify the rate of, and factors associated with, early hospital readmission at 7 and 30 days, and whether geriatrician-led home visit was associated with reduced frequency of unplanned readmission.
Methods: We performed a retrospective study of geriatric medicine patients aged ≥ 65 admitted over a 12-month period with back pain.
Results: Amongst 220 patients with back pain, the most common discharge diagnoses were vertebral fracture (36%, 79/220) and osteoarthritis (25%, 55/220). Twenty-five patients (11%) received a geriatrician-led post-discharge home visit and the remaining 195 patients received usual care through their general practitioner. Sixteen patients (7%) were readmitted within 7 days of discharge, all in the cohort who did not receive a home visit, and 52/20 (24%) were readmitted by day 30. On univariate analysis, infection causing back pain (OR 29.00, p = 0.01) and referral for Transitional Aged Care Program (TACP) (OR 3.67, p = 0.04) were both associated with 7-day readmission. On multivariate analysis, only infection as cause of back pain (OR 24.61, p = 0.01) maintained an independent association with odds of 7-day readmission.
Geriatrician home visit was not associated with 7-day (OR > 100, 95% CI 0–>100, p = 0.23) or 30-day (OR 0.97, 95% CI 0.31–3.02, p = 0.96), readmission.
Conclusion: In this retrospective study with limited numbers, early readmission was common, but a geriatrician-led model with home visit post-hospital discharge was not associated with reduced early hospital readmission. Other models beyond doctor-led interventions require consideration.
Low back pain is a leading cause of illness, pain, and disability among older adults worldwide [1]. It is associated with significant morbidity including reduced self-perceived health status, psychological distress, and poor quality of life [2]. It has a significant economic and disease burden, accounting for 1.8% of total Australian healthcare expenditure in 2008–9 [3]. In 2014–15, the prevalence of chronic back pain among older Australians aged 65 years and above was 27% [3]. Compared to working-age adults, older adults are more likely to develop severe and chronic low back pain [4] increasing their risk for poor treatment outcomes and functional disability, with a number of studies reporting negative effects on cognition, mobility, functional status, social engagement, nutrition, and sleep [5]. For this reason, the effective and timely management of low back pain in older adults is crucial.
Increasingly, older Australians are being hospitalised for low back pain, with the highest rates observed in the 80–84 age group [2]. Older adults are also particularly vulnerable to adverse clinical outcomes and complications following an episode of acute hospital care [6]. Geriatric syndromes including delirium, falls, and subacute functional decline commonly occur as older patients transition between the inpatient and outpatient setting. This frequently results in early hospital readmission, which has been recognised as a strong risk factor for mortality in older patients [7]. Readmission represents an important patient safety outcome and has been used as a measure of quality of care for older patients [8,9].
The experience of low back pain in older adults can be influenced by multiple factors including dementia, physical and psychiatric comorbidities, maladaptive illness behaviour, and age-related physical and psychosocial change [4]. Interventions which can potentially address these factors, such as community-based aged care specialist services, may help. Comprehensive Geriatric Assessment (CGA) is a holistic process designed to create a coordinated plan for older individuals by considering their medical, psychosocial, and functional influences. The benefits of CGA has been established in many meta-analyses, although not specifically in patients living with back pain [10,11]. Randomised controlled trials have shown positive outcomes including a reduction in mortality, hospital readmission, healthcare utilisation, disability, and nursing home admission [12]. With the ageing of the population in Australia and other countries, identification of risk factors associated with readmission in older people, and interventions which may reduce same, will become increasingly important.
In this context, we aimed to identify the rate of, and factors associated with, early hospital readmission at 7 and 30 days in older people with back pain, including the potential association with geriatrician-provided home visit.
We performed a retrospective cohort study at Liverpool Hospital, a tertiary university hospital in Sydney, Australia. Patients aged ≥ 65 years admitted with low back pain between May 2018 and May 2019 under Geriatric Medicine were eligible for inclusion. Patient eligibility was determined through the Clinical Information Department using the Diagnostic-Related Group code specific for low back pain. Exclusion criteria were (a) patients admitted from a residential aged care facility (RACF) (b) patients whose clinical information were not available on the hospital electronic medical record system (eMR).
Data Collection and DefinitionsA broad range of clinical documentation from the eMR was reviewed, including medical, nursing, and allied health reviews, discharge summaries, pathology, and imaging reports.
The following data was extracted: demographics (sex, age, cultural background), level of carer support (lives with others, community services), number of prescription medications, medical background, existing diagnosis of dementia or psychiatric disorder, documented episode of delirium during admission, discharge diagnosis, in-hospital back pain management practices, and clinical outcomes (discharge destination, readmission to hospital within 7 and 30 days).
Culturally and linguistically diverse (CALD) status was determined by country of birth, and defined as patients born outside of Australia and countries where English is the primary language spoken (New Zealand, the UK, Ireland, the United States of America, Canada or South Africa) [13]. Decline in mobility was determined by documented functional assessment or requirement of a new mobility aid in the month preceding hospital admission. Polypharmacy was defined as five or more concurrent regular medications, whilst hyperpolypharmacy was defined as the concurrent use of ten or more prescribed medications [14]. Calculation of the total Charlson Comorbidity Index (CCI) score was based on age and medical background [15]. The Clinical Frailty Scale (CFS) was extrapolated from the combined evaluation of domains including comorbidity, function, and cognition [16]. Dementia was defined as a chronic decline in cognitive function that causes impairment of a person’s previous level of social and occupational functioning [17]. Psychiatric disorder was defined as a behavioural or psychological syndrome that results in clinically significant distress or disability [18].
Patients deemed suitable for or likely to benefit from a post-discharge home visit were referred by their treating geriatrician to the community geriatrics service. Like many clinical services, referral to same depended on the treating team selecting the patient- the only eligibility criteria were community residence, and agreement to accept visit. The initial assessment component (doctor-led) of CGA comprised of clinical history taking (either from the patient or collateral history), physical and mental state examination, cognitive screening, frailty assessment, functional review, and medication reconciliation; this was a single visit. Visits happened within a week of discharge. A coordinated plan was developed and communicated with the patient, next of kin, and general practitioner, and referrals to community-based allied health clinicians were arranged for those patients requiring further multidisciplinary involvement. Patient education and counselling was also provided. Adherence to geriatrician-provided recommendations and/or multidisciplinary plans was not assessed.
For those that received a post-discharge home visit, additional information was obtained on clinical outcomes including delirium, falls, polypharmacy, and opioid-related complications. The incidence of these geriatric syndromes was determined on clinical history or the patient’s status at the time of their home visit. The Confusion Assessment Method (CAM) was used to screen for delirium [19].
In-hospital back pain management practices were assessed in terms of imaging modality performed, choice of analgesia, involvement by a physiotherapist, review by acute and/or chronic pain team, use of interventional radiology, surgical intervention, and referral to a community-based exercise program or TACP. TACP involves a multidisciplinary team delivering short-term, goal-oriented restorative care to optimise the functioning and independence of older adults after discharge.
Outcome MeasuresWe assessed rates of readmission at 7 days, and 30 days, to any of the hospitals within our local health district, which includes 5 acute hospitals.
Statistical AnalysisDescriptive statistics outlined demographic information, clinical characteristics, clinical management, and clinical outcomes. Frequency was used to describe categorial variables and compared using Chi-squared tests; Fisher’s exact test was used if cell size < 5. Continuous variables were described as mean and standard deviation or median and interquartile range as appropriate, and compared using the two-sample t-test or Wilcoxon Rank Sum Test respectively. Univariate and multivariate logistic regression analyses of variables potentially associated with any 7-day or 30-day readmission were performed. Variables that were significantly associated with outcome measures on univariate analysis were selected for inclusion in multivariate models.
Statistical analyses were performed using Stata® v13.0 (StataCorp, TX, USA).
In total, 248 patients were admitted with low back pain under Geriatric Medicine over the 12-month period; 28 patients were admitted from RACF and were excluded. The remaining 220 patients were included in the analysis (Figure 1). No patients were lost to follow up.
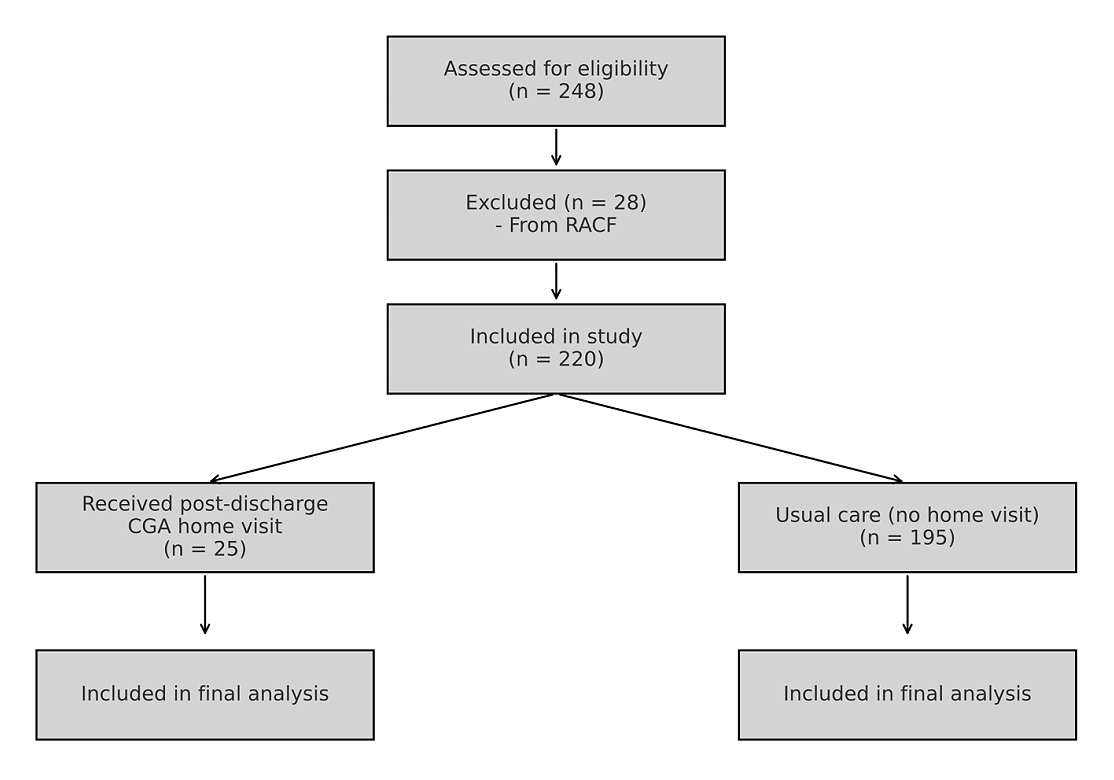 Figure 1. CONSORT diagram with inclusions and exclusion.
Figure 1. CONSORT diagram with inclusions and exclusion.
Patient demographics and admission details are summarised in Table 1. Overall, 64% were female and the mean age was 83.4 years, which was similar between those who did or did not receive geriatrician home visit. Two-thirds of patients lived with others and 39% received community services. Overall, 87% of patients experienced a decline in mobility in the month preceding their admission. Overall rates of any polypharmacy in both groups were 80%. Most patients had multimorbidity with a median total CCI score of 5, including 48% with a diagnosis of dementia and 30% with a psychiatric disorder. The median length of stay (LOS) was 10 days (IRQ 4–22).
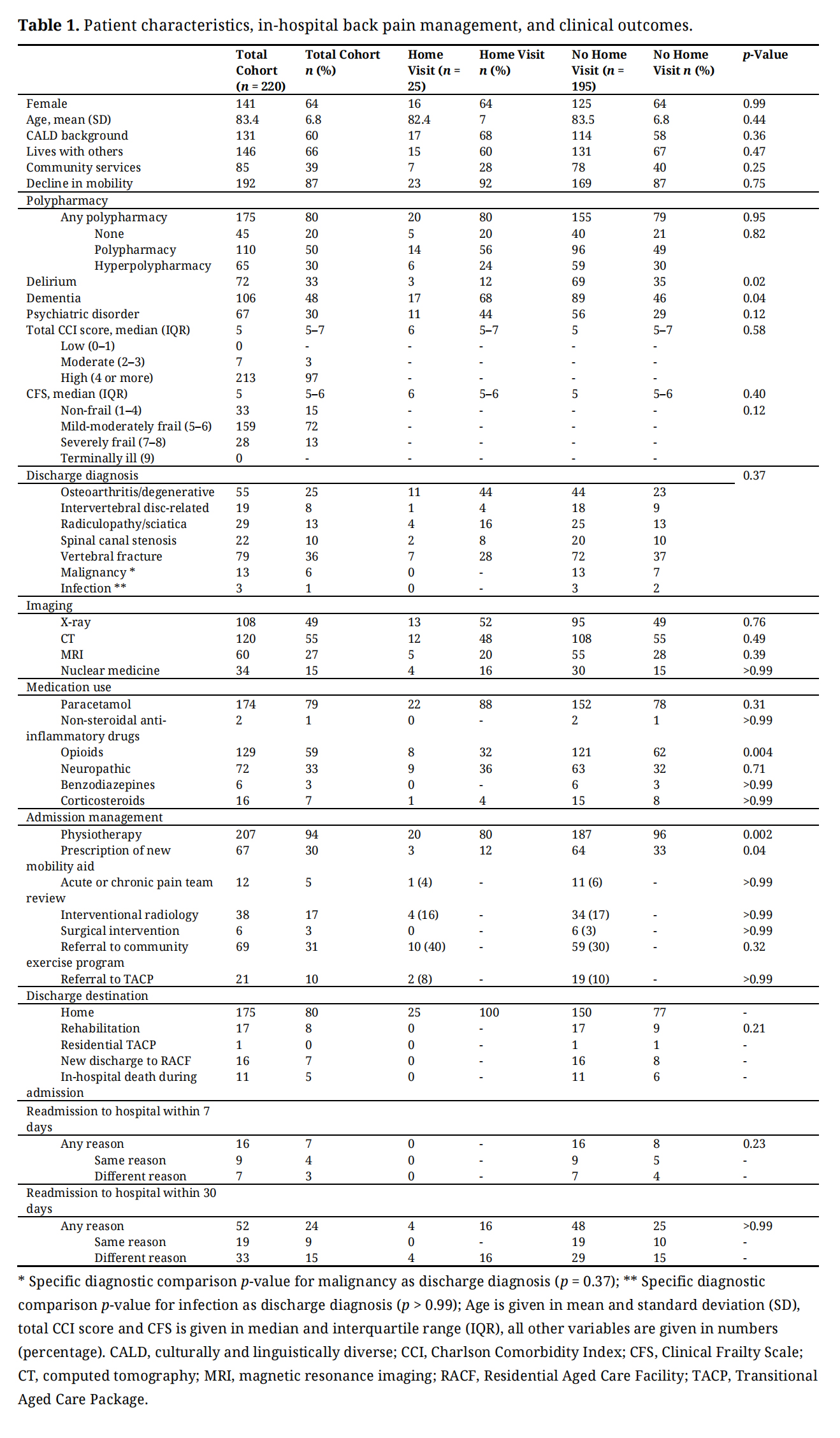 Table 1. Patient characteristics, in-hospital back pain management, and clinical outcomes.
Table 1. Patient characteristics, in-hospital back pain management, and clinical outcomes.
Twenty-five patients received a CGA home visit. Patients who received a home visit were less likely to be diagnosed with delirium during their hospitalisation but were more likely to have a diagnosis of dementia, and they had a shorted length of stay (Table 1).
The most common discharge diagnoses were vertebral fracture, followed by osteoarthritis, radiculopathy/sciatica, spinal canal stenosis, and intervertebral disc-related pathology (Table 1). X-ray (plain film) and computed tomography were the most commonly used imaging modalities. Paracetamol and opioid analgesics were prescribed in 79% and 59% of patients respectively. Overall, 33% of patients received neuropathic pain medications (amitriptyline, pregabalin, gabapentin). Non-steroidal anti-inflammatory drugs, benzodiazepines, and corticosteroids were infrequently administered. Ninety-four percent of patients received physiotherapy during admission. One in ten were referred to TACP to receive ongoing multidisciplinary intervention after discharge.
Four-fifths of admitted patients (175/220) were discharged directly home, and 8% (17/220) of patients were transferred to inpatient rehabilitation. The remainder were discharged de novo to RACF (16/220) or died during admission (11/220).
OutcomesOf the 220 patients, early hospital readmission within 7 days of discharge occurred in 16 patients (7%), all in the cohort who did not receive a CGA home visit. Unplanned readmissions at this time point commonly echoed the index hospitalisation.
On univariate analysis, factors associated with hospital readmission within 7 days included infection as the primary discharge diagnosis for back pain (OR 29.00, p = 0.01) and referral to TACP (OR 3.67, p = 0.04) (Table 2). There was no significant association between 7-day readmission and any of the following factors which we had hypothesised might increase risk: age (p = 0.46), CALD background (p = 0.19), dementia (p = 0.88), delirium (p = 0.67), psychiatric disorder (p = 0.24), polypharmacy (p = 0.42), length of stay (p = 0.78) or receipt of community services (p = 0.66).
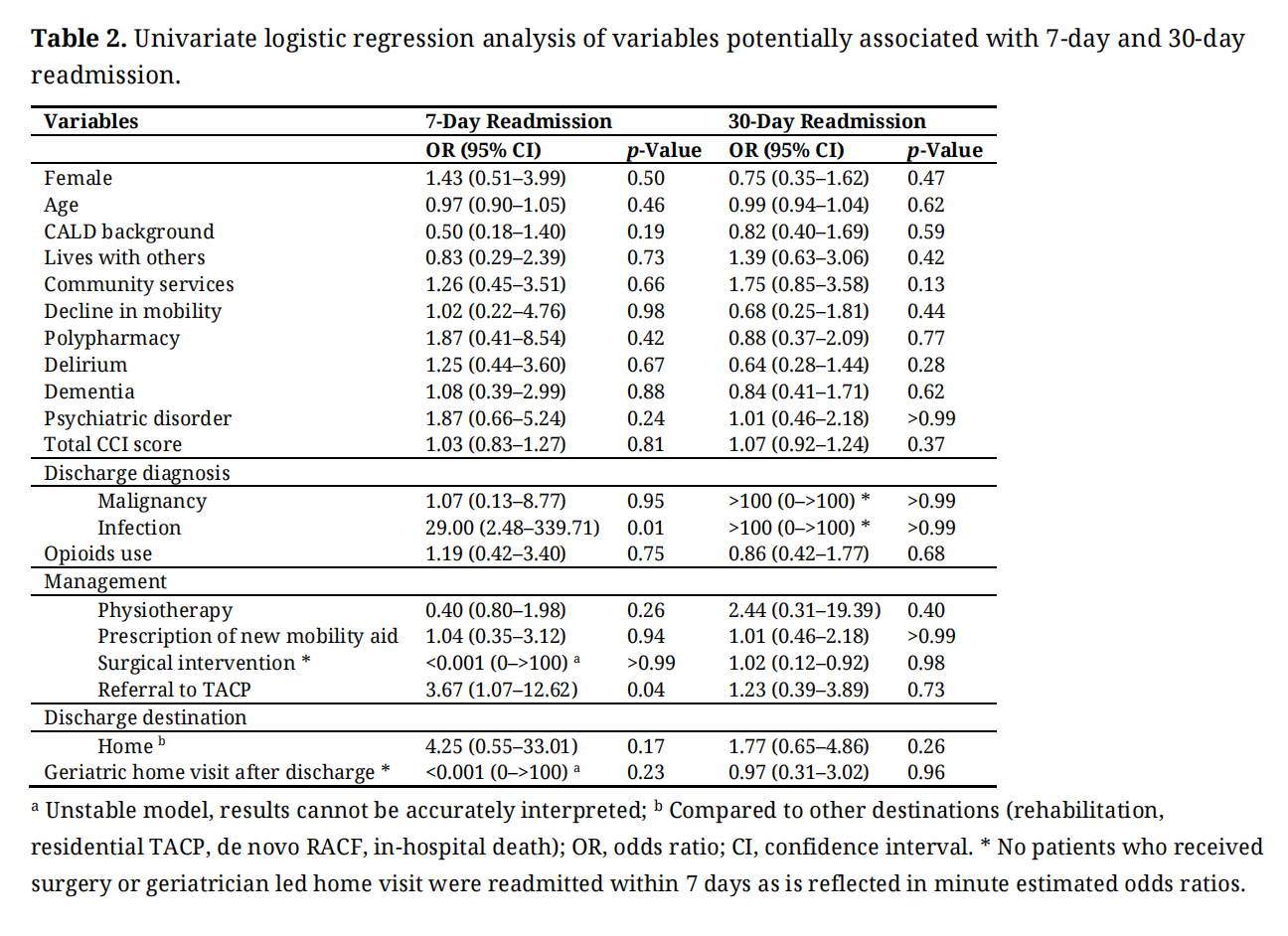 Table 2. Univariate logistic regression analysis of variables potentially associated with 7-day and 30-day readmission.
Table 2. Univariate logistic regression analysis of variables potentially associated with 7-day and 30-day readmission.
Although our overall outcome numbers were low, we attempted multivariate logistic regression analysis. Including both infectious aetiology of back pain and TACP use in the model, infectious aetiology maintained an independent association (OR 24.61, p = 0.013) with odds of 7-day readmission. Use of TACP did not maintain an association (OR 3.25, p = 0.078). These finding were unchanged when CGA home visit was forced into the model (noting that our outcome numbers were also relatively low, and inclusion of three variables in the model suboptimal).
Almost a quarter (24%) of patients were readmitted within 30 days of discharge from hospital (Table 1). There was no difference in frequency between those who did or did not receive a home visit, although the absolute proportion appeared slightly lower in those receiving a geriatrician home visit (16%, 4/25 > 25%, 48/195, p > 0.99). In both groups, recurrent back pain was an uncommon reason for readmission (Table 1). Factors such as delirium, dementia and in-hospital length-of-stay were not associated with 30-day readmission (all p > 2.8).
On univariate logistic regression analysis, a geriatrician-led home visit after hospital discharge was not associated with odds of hospital readmission at 30 days (OR 0.97, p = 0.96) (Table 2). Findings were similar when the analyses were limited to those discharged directly home and not, for example, to rehabilitation. In the cohort who received a geriatrician-led home visit (N = 25), geriatric syndromes in the post-discharge period were commonly encountered (Table 3). These included delirium (16%), new fall (20%), new polypharmacy (20%) and hyperpolypharmacy (40%), and opioid related complications (33%). These were not associated with readmission by 30 days (p > 0.1 for all, data not shown; note, no patients receiving a home visit were readmitted by 7 days, so association at this time point not analysed).
 Table 3. Clinical outcomes and polypharmacy amongst older adults who received geriatrician-led home visit (N = 25).
Table 3. Clinical outcomes and polypharmacy amongst older adults who received geriatrician-led home visit (N = 25).
As per our a priori statistical approach, multivariate analysis was not performed as none of the other investigated factors were associated with 30-day readmission on univariate analysis.
This study suggests that in community-dwelling older adults with low back pain, early hospital readmission was common. Few factors that we explored were associated with increased likelihood of readmission, except for infectious aetiology of pain, meaning that readmission may be difficult to predict. We note that the association we observed between infectious aetiology and 7-day readmission was based on small outcome numbers, and so must be interpreted with caution. A post discharge geriatrician-delivered CGA was not significantly associated with a reduced rate of unplanned hospital readmissions, when compared with usual care. While subject to the obvious selection bias of clinician-directed referral, and limited CGA, we believe that this study offers insights into real world experiences, although acknowledging that with larger numbers, the findings may have changed.
Concerningly, one in 14 (7%) was readmitted within a week of discharge, and almost 1 in 4 patients (24%) had an unplanned hospital readmission within 30 days of discharge in this study. Previous studies have shown readmission rates in older people with undifferentiated presentations between 7.4% and 23%, however these studies were not specific for low back pain [20,21]. In an Australian study of patients recently hospitalised with back pain, Kyi et al found a lower 30-day readmission rate of 11% [22], but in a cohort that was younger, less frail, less culturally and linguistically diverse, and with a lower burden of comorbidities. We also note that the experience of low back pain may be influenced by various age-related physical, psychological, and cognitive changes [4], which may predispose to unplanned readmission and be beyond the impact of a single home visit. In one retrospective cohort study, the presence of pain itself was identified as a risk factor for very early readmission within one day of acute care discharge [23]. We note that infectious aetiology for back pain was associated with increased likelihood of readmission, meaning that additional supports, or counsel to patients about this risk, may be required for these patients.
Post-discharge CGA with a nurse-led model has also generally failed to impact short-term reductions in hospital readmissions of older patients [8,24]. On the other hand, multidisciplinary transitional care programs have shown benefit in reducing readmissions in high-risk older patients [25,26]. There is currently no established uniform model of CGA. Depending on which components are used, they can be effective in reducing unplanned admissions for up to 12 months [21]. Our study was based on a newly developed community geriatrics service model, in that case management of the patients was overseen by the geriatrician. Referrals to community nursing and allied health services were arranged based on the geriatric assessment. We unfortunately did not capture whether recommendations were followed, and which allied health plans were enacted, if any. Whilst a geriatric assessment may have been a reasonable starting point for holistic patient evaluation and management, a more comprehensive multidisciplinary model may be more effective. Furthermore, this CGA model relied both upon the patient’s general practitioner actioning recommendations, and the availability of community-based allied health services, and delays therein may have adversely impacted on any potential benefit. It is also important to note that in settings where resources might be different or limited, either in terms of specialist input, or enacting multidisciplinary interventions, such a service might need to be modified. For example, in a rural setting in Ireland, O’Sullivan et al. demonstrated that a Community Specialist Team delivering CGA in primary care was feasible and associated with maintenance of functional status and low rates of hospitalisation and residential care admission [27].
We note that in our study, patients who were received a CGA home visit were more likely to have dementia, were less likely to receive opioid analgesics, and were in hospital for a shorter duration, any of which may increase risk of unplanned readmission, and given our numbers, it is quite likely we were underpowered to detect associations between other patient factors and readmission, including potentially dementia. On the other hand, it may be that patients who had pre-existing dementia are better set-up with community services, or had advance care plans put in place to reduce future readmissions.
Geriatric syndromes were prevalent in the cohort of older adults who received a home visit after hospital discharge, although due to lack of post-discharge assessment in the non-home-visit group, we cannot comment on differences between groups. Previous studies have reported rates of falls in older people in the first month after discharge of around 15% [28,29], but back pain may increase risk of falls and explain the slightly higher rate we observed. A large proportion of patients (60%) experienced new polypharmacy and hyperpolypharmacy following hospital discharge, consistent with Corsonello et al., who concluded that there was a trend towards increasing drug prescription in seniors following hospitalisation [30]. Sustained use of opioid analgesics remained high in this cohort, emphasising the importance of follow-up arrangements to monitor for opioid-related complications, as well as to ensure tapering or cessation of opioids once they were no longer required [31]. The small sample size meant that there was not enough power to detect a significant association between these clinically important outcomes and hospital readmission.
We acknowledge the limitations of this study. This was a single-centre study, which limits the generalisability of results, and the retrospective design necessitated reliance on routine documentation, which can be inconsistent or incomplete. Referral for the geriatrician CGA home visit was based on treating team referral, certainly subject to selection bias, but reflective of how many real-world clinical services function. While we included readmission to surrounding hospitals within our local health district, we acknowledge the slight chance that patients could have been admitted to hospitals outside this geographical area. The sample size in the cohort that received a post-hospital discharge CGA was small (n = 25) meaning that we may have been underpowered to detect relevant associations with this particular intervention (type II error). Review of electronic clinical documentation and post-hospital discharge home visits were attended by a single reviewer who was not blinded to the study premise, introducing the potential for confirmation bias. To minimise this effect, we used pre-specified definitions and a standard data collection sheet. Finally, we did not collect patient reported experience measures, which would have added depth to our study. Strengths include the inclusion of consecutive patients, minimising selection bias, lack of loss to follow up, and the use of real-world data, reflective of outcomes in day to day practice.
In this real-world exploratory study of community-dwelling older adults admitted with low back pain, early readmission was common, highlighting that older adults are at high risk of poor clinical outcomes in the transitional period after hospital discharge. A geriatrician-led CGA model comprising of post-hospital discharge review did not lower hospital readmission rates when compared with usual care. Further research in this field may require a large, multi-centre prospective trial to evaluate the impact of targeted interventions, including, for example, a multidisciplinary model, beyond geriatrician review alone, and incorporating CGA, as well as interventions focusing on subgroups such as those with infectious disease, in order to optimise the clinical outcomes and experiences of community-dwelling older adults with back pain.
This study was approved by South Western Sydney Local Health District Human Research Ethics Committee. Approval number: Human Research Ethics Committee (HREC) Reference No. 2019/ETH12514; Site Specific Application (SSA) Reference No. 2019/STE16206.
Declaration of Helsinki STROBE Reporting GuidelineThis study adhered to the Helsinki Declaration. The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) reporting guideline was followed.
The dataset of the study is available from the authors upon reasonable request and with additional approval from the Human Research Ethics Committee.
Conceptualization, AH, DC; Methodology, AH, DC; Formal Analysis, AH, DNC, FT; Writing—Original Draft Preparation, AH, DC, DNC; Writing—Review & Editing, AH, DC, DNC, FT.
The authors report no conflicts of interest.
No specific funding received.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
Huynh A, Conforti D, Tahir F, Chróinín DN. Management and clinical outcomes of community-dwelling older adults with low back pain: A retrospective cohort study. Adv Geriatr Med Res. 2025;7(3):e250018. https://doi.org/10.20900/agmr20250018.

Copyright © Hapres Co., Ltd. Privacy Policy | Terms and Conditions




