Location: Home >> Detail
Adv Geriatr Med Res. 2026;8(2):e260008. https://doi.org/10.20900/agmr20260008
 ,
Jayanta Gupta 2
,
Jayanta Gupta 2
1 Department of Rehabilitation Sciences, Florida Gulf Coast University, Fort Myers, FL 33965, USA
2 Department of Health Sciences, Florida Gulf Coast University, Fort Myers, FL 33965, USA
* Correspondence: Denise Allen
Over 80% of older adults take at least one prescription medication. Mild cognitive impairment (MCI) is a risk factor that may lead to unintentional errors in medication management. Identifying clients with MCI who are at risk of unintentional medication errors after discharge can allow for discharge planning to help prevent adverse events or rehospitalization. A convenient sample of 19 acute care clients with no known cognitive impairment were tested with the Montreal Cognitive Assessment (MoCA), the Rapid Cognitive Screen (RCS), and the Pillbox Test to assess the viability of a screen to identify MCI and its correlation with medication errors. Spearman rank correlation coefficient with Fisher’s z Transformation (zs) was used to describe the strength and direction of the relationship between the tests. There were significant correlations between the MoCA and the RCS (zs = 0.67 (95% CI: 0.30 to 0.86); p = 0.001), between the MoCA and the Pillbox Test (zs = −0.48 (95% CI: −0.78 to −0.003); p = 0.04) and between the RCS and the Pillbox Test (zs = −0.57 (95% CI: −0.83 to −0.13); p = 0.01). There may be efficacy in using a screen to help identify clients at risk of medication errors to help guide further testing and discharge planning.
In patients over the age of 65, more than 88% use at least one medication and 66% use three or more [1]. Over half of patients with chronic diseases are non-adherent to their medication regimens after one year [2]. This non-compliance leads to secondary health issues including additional visits to doctors and emergency rooms, as well as rehospitalizations and premature deaths [3,4]. Upwards of 20% of readmissions within 30 days to the hospital are older adults with up to 64% being medication related [5]. This can lead to costs up to $44,000 per year for each patient [6]. Medication management in older adults can be more complicated due to multiple morbidities, polypharmacy, living alone, changes in medication regime, and cognitive impairment [7–9]. Many admissions due to medication management errors are potentially preventable [9].
Medication errors by the client can be intentional or unintentional. Intentional errors may include choosing to stop medications due to side effects or costs. Unintentional medication errors can occur anywhere in the routine of medication management including communication with the physician about medications, filling prescriptions, reading directions and taking medications appropriately and getting refills as needed [10]. Unintentional errors have been found to be as high as 50% in older adults after discharge from the hospital [11].
Although a multi-disciplinary approach for medication management is recommended [12,13], clarifying each profession’s contribution to preventing unintentional errors is essential. In acute care settings, nurses and pharmacists monitor side effects, check drug interactions, reconcile medications, and assure patient understanding. Occupational therapy practitioners (OTPs), whose scope of practice encompasses health management, offer a complementary perspective by addressing cognitive, environmental, and behavioral factors influencing medication safety [11]. OTPs are positioned to screen at risk clients for mild cognitive impairment (MCI), which is often underrecognized and linked to difficulties with instrumental activities of daily living, such as medication management [7,14–16]. Once identified, OTPs then can incorporate interventions or contribute toward discharge planning to reduce adverse consequences of medication errors.
Acute care stays are brief and subtle cognitive changes can go unnoticed [17]. Clients with risk factors such as advanced age and polypharmacy may not receive cognitive or functional assessments unless deficits are obvious. Medication reconciliation and education alone may not be enough to prevent errors once clients return home. Screening at risk clients for MCI can guide further assessment decisions to inform goals and discharge planning. OTPs are well positioned to provide MCI screening, guiding interventions and ensuring informed transitions to other settings. Since comprehensive cognitive or functional medication assessments are impractical for all older adults, a brief screen targeting memory and executive function, the two cognitive domains most correlated with errors in instrumental activities of daily living [7], should be considered.
This pilot study was conducted with the aim of determining the efficacy of a cognitive screen to identify clients with possible MCI, to better guide assessment, interventions and discharge planning to prevent adverse events including readmissions due to medication errors. The two research questions were: (1) Does the Rapid Cognitive Screen (RCS) correlate with the Montreal Cognitive Assessment (MoCA) and (2) Does the Pillbox Test correlate with the MoCA and/or the RCS?
The MoCA and Mini-Mental Status Exam (MMSE) are the most common cognitive assessments reported being used by OTPs [18]. The Montreal Cognitive Assessment version 8.1 in English was chosen as the standard to compare to the cognitive screening tool. The MoCA covers seven aspects of cognition including executive function and memory and has been found to be a better assessment to distinguish between MCI and no cognitive impairment than the MMSE [19,20]. Sensitivity and specificity of the MoCA were 90% and 87% respectively if using a cutoff score ≤26 for MCI [20].
The RCS includes 3 items from the Saint Louis University Mental Status (SLUMS) exam: recall, clock draw, and insight [21]. This test reflects the same types of tests used on the MoCA for memory and executive function and takes less than 3 min to administer. The RCS shows good specificity and sensitivity for MCI compared to some other brief screening tools [21] and good validity compared to the MoCA for predicting cognitive impairment [22].
The Pillbox Test is a functional pill sorting task that requires all aspects of the four-factors model of executive functioning-action/self-regulation, planning/attention, volition/inhibition, and effective performance/self-monitoring [23]. The test consists of a weekly pillbox with four daily slots for morning, lunch, dinner and bedtime and five pill bottles with the five most common directions determined through chart reviews. A passing score cutoff was established by the test creators at 3 errors or more as determined by consultation with physicians to determine a minimum number of errors that may result in complications. A time limit of five minutes was given for the test but not clearly explained how it was determined [23]. The test shows good criterion and convergent validity and sensitivity of 75% and specificity of 80%. It is an ecological measure that mirrors actual performance clients may have with understanding and organizing medications [23].
Four researchers were trained in all three assessments and completed three calibration checks to ensure consistent administration and scoring. Any scoring discrepancies were resolved through group consensus. With approval by the hospital system IRB, researchers were assigned to different practice areas in acute care with clients that were not considered neurologically impaired, including cardiac and general medical units. Hospital staff helped identify clients who fit inclusion and exclusion criteria. Inclusion criteria included clients over 55 years with no known cognitive impairment that took at least two medications and managed them at home independently. Exclusion criteria were clients with any known or likely cognitive impairment such as clients with a stroke, dementia, or head injury. They were also excluded if clients were less than 24 h out of anesthesia or a health care provider had noticed any marked changes in cognition. Exclusion criteria also included any physical limitations that would affect client’s ability to complete paper/pencil tasks or medication sorting task including tremors, low vision, or education level below fifth grade. Clients identified as fitting inclusion criteria were asked for written consent after a description of the research was provided. Three tests were given in the following order to consenting clients: MoCA, the Pillbox Test, and the RCS. Tests were given in the order of hardest to easiest with a break provided between cognitive tests. This order was designed to help compensate for any fatigue that may worsen scores on later testing and to prevent confusion between similar components on both cognitive assessments.
Statistical analysis: Descriptive statistics are presented as mean (standard deviation) for continuous variables and number (%) for categorical variables. Spearman rank correlation coefficient with Fisher’s z Transformation (zs) was used to examine the correlation between study variables. All analyses were performed with SAS statistical software (version 9.4, SAS Inc., Cary, NC, USA).
A convenient sample of 19 clients in acute care were recruited based on inclusion and exclusion criteria. Selected demographic and clinical characteristics of study participants are displayed in Table 1. Diagnostic categories included general medical (11), cardiovascular (6), and respiratory (2).
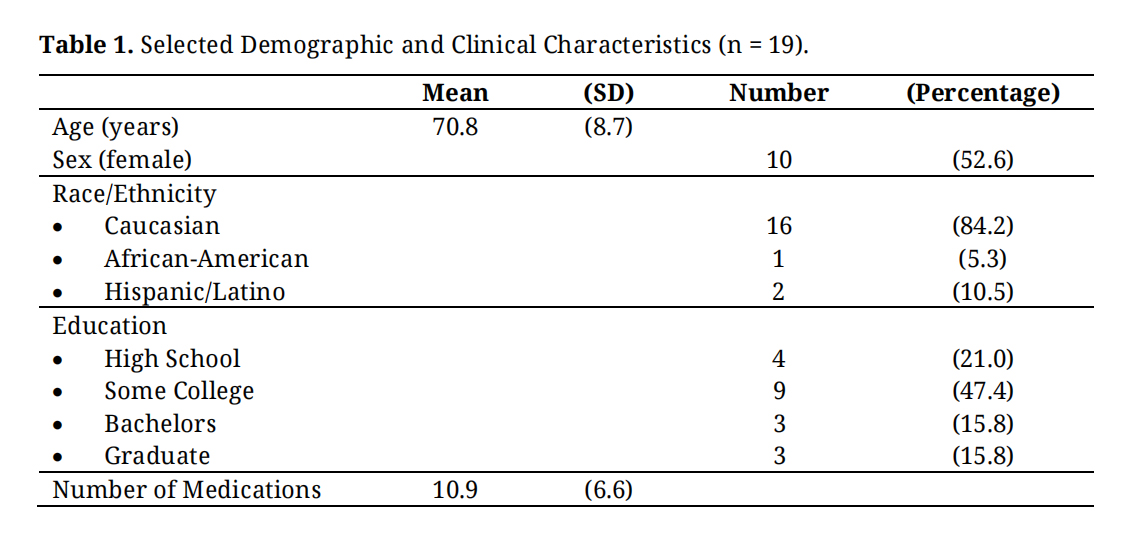 Table 1. Selected Demographic and Clinical Characteristics (n = 19).
Table 1. Selected Demographic and Clinical Characteristics (n = 19).
The MoCA indicated that 63% of participants had some form of cognitive impairment using the cut-off scores of 19–25 for MCI and ≤19 for dementia [20], 42% of participants met criteria for MCI and 21% for dementia. The RCS cut-off scores (6–7 for MCI and 0–5 for dementia) [21] gave a higher incidence of clients falling into the dementia category (37%) and lower incidence of mild cognitive impairment (16%) when compared to the MoCA.
Does the RCS Correlate with the MoCA?There was a strong positive correlation between the MoCA and RCS overall scores (Table 2). There was a moderate positive correlation between the MoCA delayed recall and RCS delayed recall (zs = 0.53 (95% CI: 0.08 to 0.79), p = 0.02) and a trend toward a positive correlation between MoCA overall memory score (MIS) and RCS delayed recall (zs = 0.47 (95% CI: −0.01 to 0.76), p = 0.047). There was no significant correlation between executive function aspects of the RCS and MoCA (zs = 0.24 (95% CI: −0.24 to 0.63), p = 0.3).
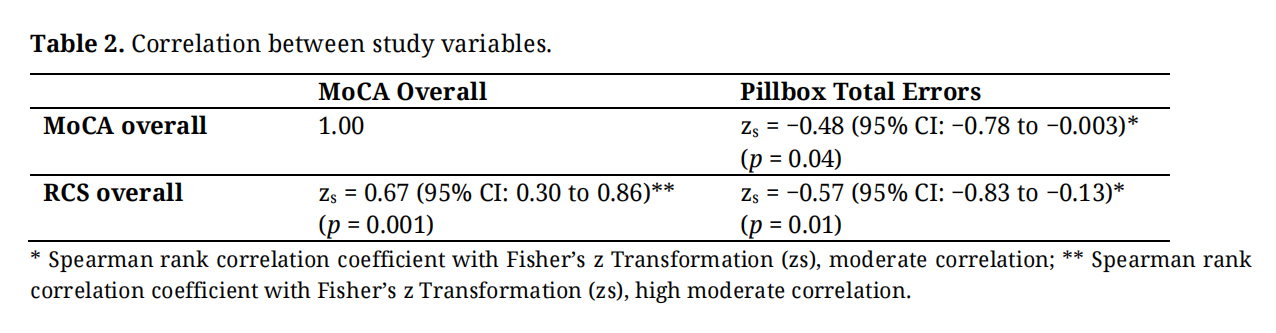 Table 2. Correlation between study variables.
Table 2. Correlation between study variables.
There were significant correlations between the MoCA and the Pillbox Test (zs = −0.48 (95% CI: −0.78 to −0.003); p = 0.04) and between the RCS and the Pillbox Test (zs = −0.57 (95% CI: −0.83 to −0.13); p = 0.01) (Table 2). Participant Pill Box Test errors were recorded at five minutes and if participants had completed the majority of the test, they were allowed to finish and total time and total errors were recorded. When extra time was given, 32% of participants went from fail to pass on the Pill Box Test. There was no significant correlation between overall MoCA and RCS scores with cognitive testing for total errors when time adjusted (for MoCA: zs = −0.44 (95% CI: −0.75 to 0.01), p = 0.05; for RCS: zs = −0.14 (95% CI: −0.56 to 0.33), p = 0.55).
These findings align with previous research linking mild cognitive impairment (MCI) to unintentional medication errors [8]. In this sample, both the MoCA and the RCS identified cognitive deficits in more than half of the clients who had no previously known cognitive concerns. This finding is consistent with prior literature indicating that healthcare professionals recognize MCI in fewer than 15% of cases [24–26]. The combined evidence suggests that without routine cognitive screening, many at‑risk individuals may have their mild cognitive impairment go undetected [27], heightening their vulnerability to adverse medication‑related events following hospital discharge.
The significant correlation between the MoCA and the RCS supports the potential utility of the RCS as a brief screening tool. The RCS classified a higher proportion of patients as meeting dementia cut-off scores compared with the MoCA; however, this discrepancy may reflect established concerns that current MoCA thresholds lack optimal sensitivity and specificity for detecting MCI [28,29]. Given the study’s small sample size, additional research is needed to further evaluate the validity of the RCS and to refine appropriate cut-off points. As with all cognitive screens, results should be interpreted as indicators for further diagnostic evaluation rather than stand‑alone evidence of MCI or functional impairment.
The study also evaluated the Pillbox Test under different timing conditions. The original five‑minute time limit, though not clearly justified in prior research [23], showed stronger associations with cognitive performance than allowing participants additional time to complete the task. Notably, when extra time was permitted, 32% more participants achieved a passing score, diminishing the test’s correlation with both the RCS and MoCA. This pattern aligns with earlier findings suggesting that individuals with MCI often require increased time to complete instrumental activities of daily living (IADLs) [30,31]. While both cognitive tests correlated with total error counts, neither correlated with the pass/fail classification based on the ≥3‑error threshold commonly associated with clinically significant medication complications [23]. Prior analyses indicate that a higher error threshold (≥5 errors) may yield better sensitivity and specificity, underscoring the need for further study to determine an appropriate and clinically relevant cutoff [23].
The RCS shows promise as a screening tool for cognitive impairment. Larger, more diverse studies are needed to validate cutoff scores, refine pass/fail criteria, and assess predictive value for medication errors. Further studies should also account for confounding factors such as specific medications. Larger, more diverse populations may also allow for more generalizability of results. Testing should also explore alternative assessments for patients that were excluded from the current study due to factors such as vision or tremors. Further investigation should also identify client factors beyond age to more efficiently identify clients who would benefit from cognitive screening [32].
Implications for Occupational Therapy PracticeThe RCS demonstrates promise as a practical screening tool for detecting cognitive impairments relevant to medication management. Occupational therapy practitioners (OTPs) can feasibly integrate such a screen into routine assessments, particularly for patients with risk factors such as polypharmacy, recent medication changes, chronic conditions, or living alone [5,7,8]. Although an MCI diagnosis can be difficult [28] and requires more than a single screen, brief cognitive screens can play an essential role in identifying individuals who may otherwise remain undiagnosed. Early identification enables OTPs to pursue further evaluation, determine the impact of cognitive changes on IADLs, and inform discharge planning to ensure adequate support. Given their holistic perspective, OTPs are well positioned to address emerging cognitive difficulties and develop interventions to maintain patient independence [11].
This study has a few limitations. It was confined to a small, convenient, homogenous sample within one hospital system. The low statistical power due to a small sample could have limited the study’s ability to detect some true effects. Most of the study participants were Caucasian (~84%) and most (~80%) had some college education. These factors introduced selection bias and limited the external validity of the study. The internal validity of the study could also have been affected to some extent. Although we attempted to account for factors that could have reduced a client’s ability to complete testing such as fatigue and effects of anesthesia, participants were not excluded due to the presence of factors that could have affected cognitive status, such as being on medications with potential cognitive side effects (Table S1). Other distractions such as noise in hospital rooms could also have influenced cognitive performance. Finally, as this was a pilot study intended to explore the feasibility of a larger study rather than test hypotheses, we did not adjust for multiple testing in the statistical analysis. In this context, our study results are more appropriately viewed as promising trends requiring validation in larger studies rather than definitive, as mentioned below.
This preliminary study provides early evidence that both the MoCA and RCS can identify previously unrecognized cognitive impairment in acute‑care patients, reinforcing the importance of routine screening to reduce risk for medication errors after discharge. The significant correlation between the RCS and MoCA supports the RCS’s potential utility as a brief screening tool, although further research is necessary to validate appropriate cutoff scores, refine pass/fail thresholds, and determine predictive value for medication‑related outcomes.
Despite sampling limitations and potential confounding factors, the findings highlight the relevance of cognitive screening within occupational therapy practice. Larger and more diverse studies are needed to confirm these results, explore the influence of medications and other clinical variables, and identify suitable assessments for patients excluded from the present study. Ultimately, early detection of MCI can guide targeted interventions, inform discharge planning, and better support safe medication management, underscoring the vital role of OTPs in promoting patient safety and independence.
The study was approved by the Institutional Review Board of Lee Health (IRB00000752, January 2023). Informed consent was obtained from all subjects involved in the study.
Declaration of Helsinki STROBE Reporting GuidelineThis study adhered to the Helsinki Declaration. The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) reporting guideline was followed.
The following supplementary materials are available online, Table S1: Diagnoses and medication of participants.
The dataset of the study is available from the authors upon reasonable request.
Conceptualization, methodology, validation, investigation, resources, data curation, writing-original draft preparation and revisions, visualization, supervision, project administration, DA. Statistical analysis, original draft preparation and revisions, JG.
The authors declare that they have no conflicts of interest.
This research received no external funding.
Thanks to the hospital staff and the students who helped with data collection to make this study possible-Madison Brown, Margaret McGee, Miranda Nelson, and Michelle Tortora.
1.

Copyright © Hapres Co., Ltd. Privacy Policy | Terms and Conditions




