Location: Home >> Detail
J Psychiatry Brain Sci. 2026;11(3):e260008. https://doi.org/10.20900/jpbs.20260008
 ,
Emily Kingsland 2 ,
Imy Shenouda 3 ,
Michelle Azzi 1 ,
Sara Hughes 1 ,
Gina Cormier 1 ,
Ayse Turkoglu 1 ,
Martin Drapeau 1,4,*
,
Emily Kingsland 2 ,
Imy Shenouda 3 ,
Michelle Azzi 1 ,
Sara Hughes 1 ,
Gina Cormier 1 ,
Ayse Turkoglu 1 ,
Martin Drapeau 1,4,*
1
2
3
4
*
Background: Cognitive behavioural therapy for depression includes cognitive and behavioural techniques to target depressive symptoms. Cognitive techniques are often separated into interventions that target automatic thoughts and those that target core beliefs. Interventions that focus on core beliefs have been presented in the literature for decades. However, a consolidated review of the available contents pertaining to interventions focusing on core beliefs when treating depression has yet to be completed. Aims: This scoping review aimed to identify and define core belief techniques and describe core treatment recommendations in the treatment of major depression. Method: A literature search was completed in three databases including PsychINFO, EMBASE and Medline. The methodology followed scoping review guidelines and a thematic analysis framework. Results: The review uncovered two clusters of techniques. The first aim to identify the core beliefs and include such techniques as reviewing the historical context for underlying beliefs, the downward arrow technique, and the use of inventories. The second aim to modify core beliefs and include techniques such as examining the evidence, exploring the advantages and disadvantages of a belief, conducting a historical test, the continuum method, and using positive data logs. Specific recommendations for using each technique are also presented.
Several techniques and interventions are used when delivering Cognitive Behavioural Therapy (CBT) for the treatment of patients with major depression. Two broad and highly common clusters of techniques that are detailed in treatment manuals are behavioural activation, and cognitive interventions [1–3]. Behavioral activation generally involves helping patients schedule activities that are positively reinforcing, whereas cognitive interventions target cognitive constructs such as automatic thoughts and core beliefs. Automatic thoughts are unstable, temporary, typically situation-specific and are often more reflexive in nature [4–7]. On the other hand, core beliefs are described as deeply ingrained beliefs that are often stable and cross-situational [7–10]. They are rigid, fundamental, and inflexible, and are therefore lasting comprehensions or representations of the individual, others, and/or the future, which have developed from early significant experiences [9,11]. From a cognitive-behavioural perspective, negative core beliefs are associated with increased vulnerability to depression [12].
Wright et al. (2006) [13,14] therefore considered such techniques to be particularly important when treating major depression, as these techniques are believed to alleviate depressive symptomology and act to prevent the impact of future stressors. Further, Alloy (1988) [15] highlighted the importance of targeting maladaptive core beliefs as they may act as a barrier to seeking and progressing in treatment. Beliefs that are held as facts without disputation can be strengthened over time and when activated can lead to a negative mood or a depressive episode (e.g., [16]). Altering and shifting beliefs to be more flexible through the use of cognitive techniques is therefore considered to be a central aspect to the treatment and prevention of depression.
Techniques that target core beliefs are often applied concurrently with techniques that target automatic thoughts. Many techniques (e.g., Socratic Questioning and examining evidence for/against a thought or belief) can also act simultaneously on both levels of cognition (e.g., [17]). However, there are some interventions that appear to be more specific to core beliefs, such as the downward arrow technique. Although previous reviews have explored strategies for behavioural activation and automatic thoughts [18], our review of the literature indicates that there is currently no review that has focused on core beliefs. Given the importance of techniques that focus on core beliefs in the treatment of depression, this gap in the literature needs to be addressed. Hence, the aim of the present review was to identify CBT strategies that target core beliefs in major depression, as well as delineate clinical recommendations for applying these techniques.
This scoping review followed the framework developed by Arksey and O’Malley (2005) [19]. While completing the 5th step of this framework (i.e., collating, summarizing and reporting the results), a thematic analysis was conducted and followed the six phases delineated by Braun and Clarke (2006) [20].
Following the Arksey and O’Malley (2005) [19] framework, the research questions were first defined. The questions addressed included: (1) What are the CBT techniques that focus on core beliefs? (2) How are these therapeutic techniques defined? and (3) What are common clinical recommendations for delivering these therapeutic techniques?
The second step of the framework consisted of identifying the relevant studies for the scoping review. A research librarian with expertise in scoping reviews was consulted by the team. A search string was developed based on previous searches used in empirical studies and similar scoping reviews. Key terms pertaining to cognitive techniques, CBT treatment manuals, types of empirical studies, and major depression were included in the search strategy (see Appendix A). The literature search was performed in three electronic databases (PsychINFO, Embase and Medline) by graduate students and a senior researcher. Records were included if they were English peer-reviewed articles, manuals, handbooks, and theoretical books that focused on adult populations (18+), major depressive disorder, and CBT therapist techniques. The search did not include grey literature for feasibility reasons. Reference lists of identified studies and manuals were reviewed to include additional potentially relevant articles in the review.
The third step of the framework consisted of selecting the studies. The selection of studies was performed by two graduate students who had previous training in conducting reviews, and one senior researcher. The reviewers worked independently then met to reach consensus. The reviewers consulted with a fourth reviewer whenever disagreements occurred. Details about the selected and excluded studies can be found in the PRISMA chart (see Figure 1).
The fourth step of the framework consisted of charting the data from the selected records. This step was independently performed by four reviewers. These reviewers then met to reach consensus. Data extraction consisted of extracting the following information from the selected records: publication type, patient diagnosis, treatment type, duration, number of sessions, demographics, and study design (See Table S1).
The fifth and final step consisted of collating, summarizing, and reporting the results. In this step, the thematic analysis was conducted using the Consensual Qualitative Method [21]. All raters had extensive training using the method. The first 10 records were reviewed jointly by the two raters working together. The reviewers then proceeded to work independently. However, 35% of records were randomly selected and jointly reviewed by the raters to reach consensus. If disagreement occurred, a third reviewer was consulted. The codes were then sorted and collated into themes and sub-themes, as presented below.
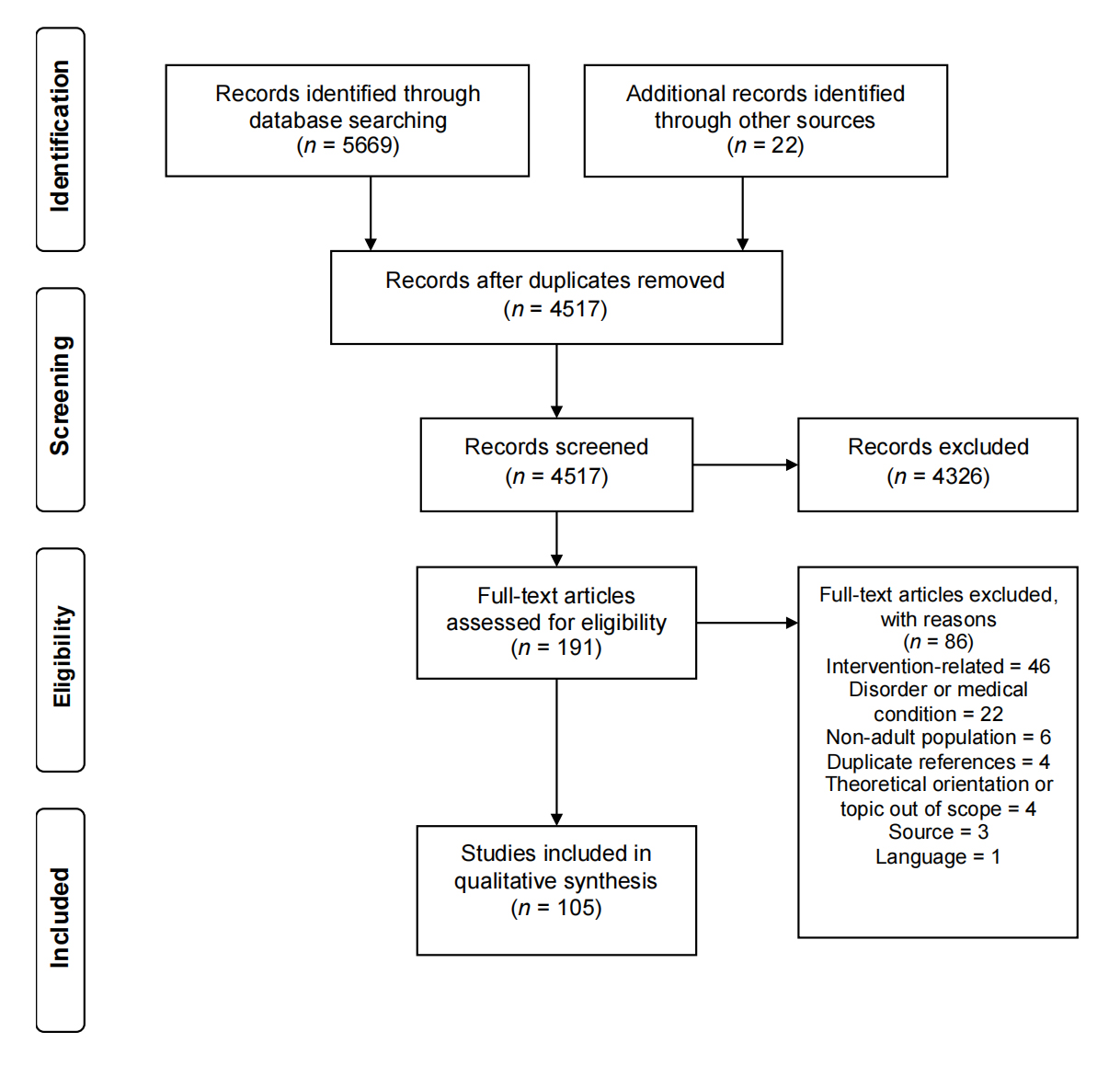 Figure 1. PRISMA Flow Diagram. This figure shows the flow chart of the scoping review (Moher et al., 2009). PRISMA stands for Preferred Reporting Items for Systematic reviews and Meta-Analyses.
Figure 1. PRISMA Flow Diagram. This figure shows the flow chart of the scoping review (Moher et al., 2009). PRISMA stands for Preferred Reporting Items for Systematic reviews and Meta-Analyses.
The thematic analysis yielded two broad themes, consisting of two overarching groups of techniques: (1) techniques that identify core beliefs, and (2) techniques that aim to modify core beliefs. Those two themes were further divided into several sub-themes of individual techniques. Moreover, the thematic analysis led to the identification of clinical recommendations pertaining to the application of the techniques. In this scoping review, the overarching group of identifying core belief techniques are first defined, as well as the individual techniques within that group. Second, the overarching group of modifying core belief techniques are defined, as well as the individual techniques within that group. Lastly, the clinical recommendations pertaining to the application of the techniques are outlined and discussed.
Techniques to Identify Core BeliefsDefinition. These are techniques that aid the patient in recognizing and pinpointing deeply engrained core beliefs. To identify core beliefs, the therapist helps the patient monitor accessible beliefs that are consistent across situations. Identification strategies assist the patient in reflecting or engaging in self-inquiry related to the meaning of a belief [22]. Another element closely linked to identifying core beliefs is the exploration of these beliefs and developing a deeper understanding of the meaning linked to a belief [23,24]. It is important to note that the identification of core beliefs begins to occur through the process of exploring automatic thoughts [25]. Techniques applied to the identification of automatic thoughts are similar to techniques denoted as integral to the identification of a core belief. The core strategies used for identifying core beliefs include understanding the historical context, using the downward arrow, and using inventories and worksheets that identify underlying core beliefs.
Historical context. Reviewing the historical context for underlying beliefs is noted as a key strategy in identifying core beliefs [11,12,14]. Berk et al. (2004) [11] define this process as exploring and discussing memories, and early formative experiences and impactful relationships and events to discern maladaptive and adaptive beliefs [14]. The therapist guides the patient to identify patterns across situations, people, mood states, and events. An important aspect to this technique is providing psychoeducation on the process of attributing meaning to past events and how people often develop rules for encoding information [26]. With the help of a therapist, these past events are then systematically reviewed for commonalities in meanings [27]. Wright et al. (2006) [14] describe it is common to incorporate guided discovery and questioning to detect recurring themes and explore the impact of significant figures, culture, socialization, interests, jobs, values and activities.
Downward arrow. The downward arrow technique has been denoted as a core and effective strategy for identifying core beliefs and assumptions [25,28]. This technique consists of a process of consecutive repeated questioning that increases the depth from an initial automatic thought to the underlying core belief [14,29]. Questions such as “if this were true, what would it mean?” are initially directed at a conscious and accessible thought; the clinician then proceeds to ask the question repeatedly in response to each given answer [30]. Through careful questioning, deeper meaning is elicited that enables the patient to delve into a fundamental belief or conviction [24]. The series of questions continues until the core belief is identified [31]. Fefergrad and Richter (2013) [32] explain that this process often elicits strong affect from the patient when the belief is identified. Therefore, this technique can also be used to identify the emotion closely associated with the core belief [33]. Moreover, this therapeutic strategy can assist in uncovering meaning, determining implications of events, and enhancing the therapeutic alliance [28,33].
Inventories and worksheets. An additional approach to identifying core beliefs is through the use of inventories and worksheets. Given that core beliefs are deeply ingrained and difficult to access, the use of an inventory can be helpful in discerning core beliefs [6,14]. Wright et al. (2006) [14] explain that the administration of assessment tools such as inventories or worksheets that identify common core beliefs can provide a level of insight that may not be easily or directly observed otherwise. O’Donohue (2008) [33] suggests incorporating the use of measures such as the Dysfunctional Attitudes Scale (DAS) [34], Personality Beliefs Questionnaire (PBQ) [35] and Young Schema Questionnaire (YSQ) [35] when identifying core beliefs. These inventories allow the patient to reflect on how well they can relate to examples of suggested core beliefs and also think about their own underlying beliefs [14,36]. These inventories also allow patients to draw contrasts between adaptive core beliefs and maladaptive core beliefs. The scales can provide a more comprehensive array of understanding the complexity of underlying cognitive processes in the patient [14].
Techniques to Modify Core BeliefsDefinition. Techniques that modify core beliefs have been described as a fundamental set of strategies within CBT [37]. Modifying techniques tend to consist of ones that examine, test, challenge and correct maladaptive beliefs of the self, others and the world [31,36]. Froján-Parga et al. (2009) [37] note that techniques used to modify automatic thoughts in CBT can also be applied to modify more deeply ingrained assumptions and core beliefs. Scholars note that the goal of modifying techniques is to restructure rigid and unrealistic core beliefs into a system that is more flexible and more in line with reality [22,38–40]. Freeman and Oster (1999) [41] further state that the goal is not to eradicate the beliefs but to reshape and shift them to be less extreme and have a more balanced perspective [38,42]. Modifying interventions consist of guidance from the therapist to activate a patient’s metacognitive skills [6]. The techniques used for modifying core beliefs include examining evidence, the advantages and disadvantages of the belief, the historical test, the continuum method, and the alternative beliefs and positive data log.
Examining evidence. Examining the evidence is a core strategy applied to core beliefs. Moore and Garland (2003) [43] suggest this is a key strategy to begin weakening beliefs and reduce the absolute acceptance of them [33]. This technique requires patients to systemically and objectively identify evidence for and against a certain maladaptive core belief, thereby calling into question the accuracy of their initial core belief [22]. The patient is guided to reduce their perseveration on the maladaptive core belief, increase the use of the objective approach, and build upon the evidence against the maladaptive core belief [14,23,43]. With this technique, the patient is encouraged to identify evidence from their own experiences [33], examine implications or consequences of holding the maladaptive belief [22,44,45], and assess the belief from many perspectives [14,46,47].
Exploring the advantages and disadvantages. Exploring the advantages and disadvantages of holding certain beliefs and assumptions is also presented as an important technique [48]. Moore and Garland (2003) [43] describe this technique as an important initial step in modifying a belief. It requires an explicit listing of the advantages and disadvantages of holding both specific adaptive and maladaptive beliefs, and of changing beliefs [43,49]. The patient then has a written record which can assist them in informing the process to modify the core belief [14,46]. Exploring the advantages and disadvantages allows the patient to participate in a cost-benefit analysis where they can analyze the relative weight of both sides and assess the short and long-term implications of holding a core belief [43,47].
Using historical tests. An additional technique that is recommended is the technique of using historical tests. Berk et al. (2004) [11] suggest that when exploring the evidence, it is important to also focus on early origins of each belief. This is intended to work as a way to begin to establish more adaptive beliefs and responses. The therapist and patient collaborate on reviewing the existing history and examining how specific instances, such as key events, specific time periods, and discrete developmental periods, may undermine the maladaptive core belief [12,38,43,50]. Persons and colleagues [38] suggest concluding the historical review by summarizing the confirming and disconfirming information for the core belief, thus giving the patient an opportunity to develop a more adaptive and increasingly flexible perspective.
Continuum method. McBride and colleagues [12] identify the continuum method as a core technique to shift absolutist beliefs to a more balanced view. Persons et al. (2001) [38] note that patients with depression tend to hold core beliefs that are global and extreme in nature. This technique allows patients with depression to notice the polarity of thinking and adopt a more dimensional approach to thinking [12,14,36]. Techniques such as examining the evidence or questioning can be applied with this technique to aid in shifting evaluations of the self towards a more adaptive or balanced stance [12].
Alternative beliefs. This technique is described as assisting the patient in developing or building alternative beliefs [43,51]. The strategy consists of creating a list of plausible and adaptive beliefs that would replace the adaptive beliefs [14,27,41]. Developing alternatives is not simply about thinking positively and substituting negative core beliefs with positive alternatives; it is about enhancing flexibility and encouraging additional ways of responding [43]. Alternative belief strategies aim to influence the foundational or basic rules that guide the patient’s thinking [14]. When considering alternate beliefs, the patient is attending to information that may have initially been filtered out or missed while developing the maladaptive belief; therefore, this technique can provide information that will counteract maladaptive beliefs and strengthen adaptive beliefs [43]. To aid in this process, the advantages and disadvantages technique can be used to help the patient consider the short and long-term implications of the initial and alternate beliefs [27]. An additional technique that can be used is the as if technique where the patient imagines what thoughts they would have if they adopted the alternative belief [27]. This provides an opportunity for the patient to examine current or potential experiences through the lens of the alternative rules or beliefs [33].
Positive data log. A positive data log is a technique applied to modify a maladaptive core belief into a positive or more balanced one [41]. This technique involves the patient and therapist collaboratively developing a data log of evidence that supports the new core belief [31,38]. The data log increases the awareness and monitoring of events that are consistent with the new core belief. The patient is tasked with pro-actively identifying information that clearly supports the new belief, encouraging the patient to notice data that may have been previously viewed as small or insignificant [12]. At the same time, the clinician encourages the patient to notice when they are discounting or resisting information that is incompatible with the more absolute or old maladaptive core belief [12,50].
Clinical Recommendations for the Application of Techniques Targeting Core BeliefsClinical recommendations pertaining to the use of techniques targeting core beliefs are commonly highlighted across CBT treatment protocols for major depression. Most clinical recommendations that were identified in this scoping review are primarily focused on the recommended timing of these techniques and particular caveats related to the nature of these ingrained structures. Another line of clinical recommendations that were commonly referenced are specific to techniques directed at identifying core beliefs and working with adaptive as opposed to maladaptive core beliefs.
Clinical Recommendation 1: Apply core belief strategies after depressive symptomology has subsided. Timing is central when using techniques that address core beliefs in major depression. Careful consideration must be given to the severity of depressive symptoms because it is recommended to use techniques that address core belief only when symptomology has begun to reduce [25]. As treatment progresses and depressive symptomology begins to ameliorate, the patient is thought to have developed enhanced resilience that is conducive to greater readiness for core belief work [27]. Dobson further advises that applying these techniques prematurely can be linked with a worsening of symptoms. Considering the level of depression in determining appropriateness of the intervention is considered to be critical in this process of clinical decision-making.
Clinical Recommendation 2: Incorporate core belief interventions in later phases of treatment. Work related to both identifying and modifying core beliefs was consistently recommended during the later phases or end of treatment [16,25,27,33]. One exception for the inclusion of core belief work earlier in psychotherapy is related to case formulation. O’Donohue (2008) discusses the importance of identifying core beliefs in early phases to inform the case conceptualization and treatment planning process. The overarching clinical recommendation indicates the importance of timing, which is consistent across studies and manuals, and through earlier and more current records [27,39].
Clinical Recommendation 3: Apply core belief interventions once there is a strong therapeutic alliance. Another recommendation is to apply these techniques in the context of a strong therapeutic relationship. Wright et al. (2006) [14] indicated that elements integral to strong rapport such as expressing empathy and acceptance are factors that can facilitate and ease the identification and modification of these more ingrained cognitive structures.
Clinical Recommendation 4: Provide psychoeducation, and normalize the slow and gradual shifting of core beliefs. Sudak (2012) [49] note the challenging nature of working with core beliefs as they are often deeply embedded into the identity of the patient and have been reinforced for years throughout the patient’s life [14]. Freeman and Davis (1990) [24] suggest that beliefs that are less compelling are often more amenable to modifications. These less ingrained core beliefs are more likely to shift with testing and modification techniques. Moore and Garland (2003) [43] emphasize the importance of providing psychoeducation to the patient on the slow process of change. Knowing that patients who struggle with depression have a tendency to engage in cognitive errors where they evaluate themselves negatively, normalizing this gradual shift in cognition will discourage them from attributing the slow progress to faults in the self.
Clinical Recommendation 5: Identify core beliefs using multiple techniques. It is recommended that therapists incorporate a variety of techniques when it comes to identifying core beliefs [31,33]. Wright and colleagues [14] noted that identifying core beliefs can occur through a developmental review of interpersonal relationships, significant events, or circumstances that are central themes or topics. Additional recommendations for uncovering core beliefs are through the administration of inventories, particularly when the patient is observed to have difficulty with noticing core beliefs. By using inventories, both positive and negative core beliefs can be identified that may have been previously dormant or difficult to detect. Other scholars have recommended identifying core beliefs through attending to language used such as use of verbs including “should” [36] and through noticing moments of strong affect [31].
Clinical Recommendation 6: Focus on both adaptive and maladaptive core beliefs, as well as on a limited number of beliefs related to the presenting problem. When working on core beliefs, Persons et al. (2001) [38] recommend selecting one to two core beliefs that appear most closely related to the patient’s presenting problems. Moreover, it is recommended that the therapist also tend to the adaptive aspects of the patient’s underlying cognitive structures, and not just the maladaptive core beliefs [14]. Shifting attention to more adaptive core beliefs can be a more effective way of producing core belief change [12]. Dobson (2008) [27] suggested that the focus on adaptive or developing of a more adaptive core belief should be a belief that is important and attainable to the patient.
This review focused on identifying cognitive techniques that target core beliefs, and aimed to identify clinical recommendations pertaining to their use. Therapist techniques applied in the treatment of major depression were reviewed from the retrieved literature. These interventions were grouped into two clusters: (1) techniques that identify core beliefs and (2) techniques that modify core beliefs. Common identifying techniques applied to core beliefs included considering the historical context, the downward arrow and use of inventories and worksheets. On the other hand, techniques directed at the modification of core belief included examining the evidence, examining the advantages and disadvantages, conducting historical tests, the continuum method, and an alternative beliefs and positive data log. In addition, the review identified a number of clinical recommendations for interventions. These recommendations included applying techniques after there has been a reduction in depressive symptomology, towards the end of treatment, and in the context of a strong therapeutic relationship. Recommendations also included normalizing the gradual shift of core beliefs and applying a variety of techniques to identify beliefs. Lastly, the review identified the importance of identifying maladaptive and adaptive beliefs and focusing on a select number of core beliefs.
The present review has strengths and limitations. First, there may have been a risk of bias during the extraction of the techniques and conduction of the thematic analysis; it is possible that other reviewers would have examined the available records differently. To mitigate this limitation, more than one reviewer was included in all steps of the process. Second, for feasibility reasons, grey literature was not considered. With regards to this study’s strengths, it is one of the first reviews to summarize the cognitive techniques used in CBT that target core beliefs in major depression. Not only does it detail the cognitive techniques, but it also provides a list of recurrent clinical recommendations found in the literature that explain how to apply the cognitive techniques. Therefore, this review combines a wealth of theoretical and practical knowledge pertaining to CBT techniques targeting core beliefs. Consequently, this scoping review can serve as a useful tool for both clinicians and researchers.
Follow-up research could examine individual techniques and the pairing of techniques to determine their effectiveness and relevance within CBT treatment protocols in reducing depressive symptomatology. Other future directions may be to begin uncovering existing empirical support for the clinical recommendations compiled in this review and test the efficiency of each. Most studies related to CBT focus on a quantitative analysis [52] and researchers have advised the importance of incorporating qualitative analyses in order to enrich and further understand therapeutic techniques [53]. This study demonstrated the importance of a scoping review to carefully uncover and clearly demonstrate the need for further studies to more systematically test these recommendations prior to implementing them in clinical practice.
Ethical review and approval and patient consent were waived for this study as they are not applicable to reviews.
Declaration of Helsinki STROBE Reporting GuidelineThis study adhered to the Helsinki Declaration. The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) reporting guideline was followed.
The following supplementary materials are available online, Table S1: Study characteristics of all included articles in the scoping review.
All data generated from the study are available in the manuscript or supplementary files.
AS: Writing–review & editing, Writing–original draft, Project administration, Methodology. EK: Database search curation and project administration. IS: Project administration, Data extraction, Writing–review & editing. MA: Project administration, Data extraction, Writing–review & editing. SH: Writing–review & editing. GC: Writing–review & editing. AT: Writing–review & editing. MD: Writing–review & editing, Supervision, Resources, Methodology, Conceptualization.
The authors declare that they have no conflicts of interest.
This research was funded internally by the McGill Psychotherapy Process Research Group.
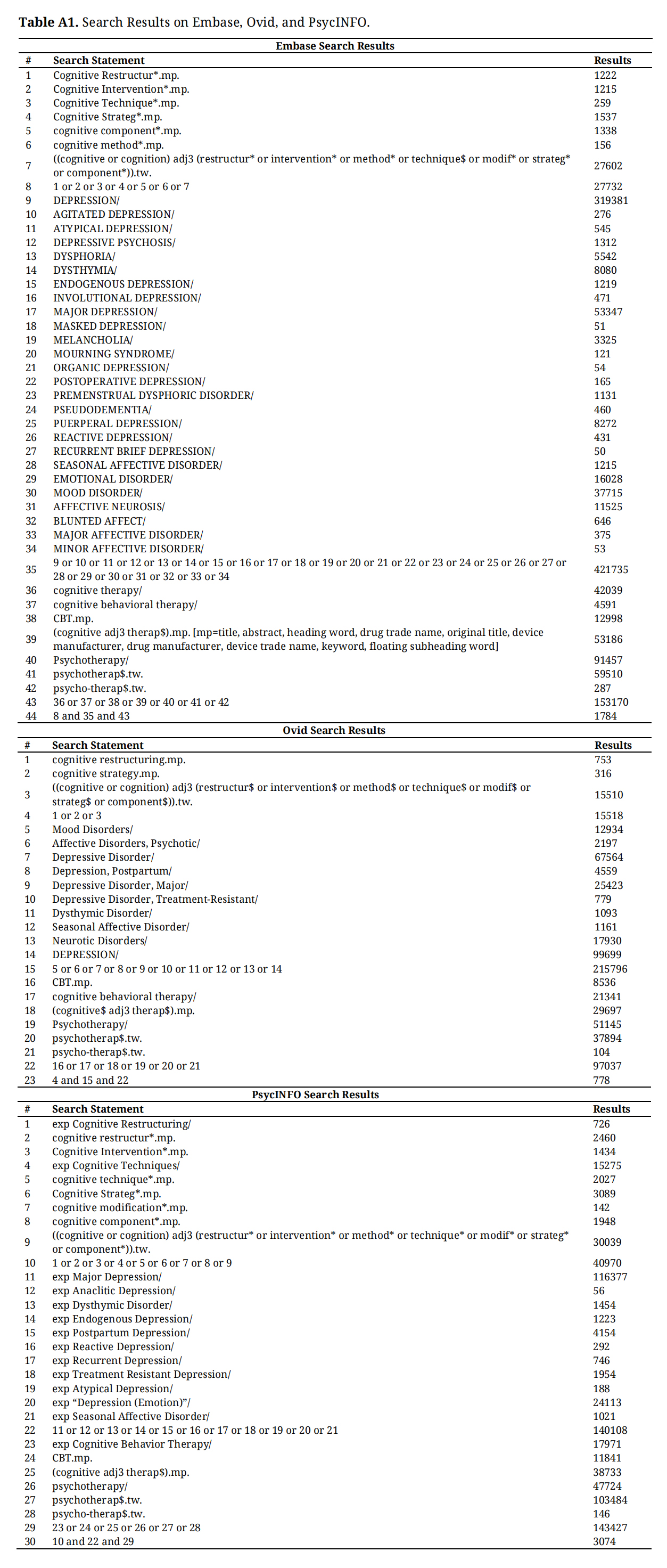 Table A1. Search Results on Embase, Ovid, and PsycINFO.
Table A1. Search Results on Embase, Ovid, and PsycINFO.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
Sheptycki A., Kingsland E, Shenouda I, Azzi M, Hughes S, Cormier G, et al. Therapist Techniques in Cognitive Behavioural Therapy: A Scoping Review of Interventions Targeting Core Beliefs in Major Depression. J Psychiatry Brain Sci. 2026;11(3):e260008. https://doi.org/10.20900/jpbs.20260008.

Copyright © Hapres Co., Ltd. Privacy Policy | Terms and Conditions




