Location:Home >> Detail
Med One. 2017; 2: e170007. https://doi.org/10.20900/mo.20170007

1 Department of Electrical, Computer, and Biomedical Engineering, the University of Rhode Island, Kingston, RI 02881, USA
2 Howard-Tilton Library, Tulane University, 7001 Freret St, New Orleans, LA 70118
3 Department of Biomedical Engineering, Tulane University. 1440 Canal St, New Orleans, LA 70112
Corresponding to: Esterlina Garcia, Department of Biomedical Engineering, Tulane University. 1440 Canal St, New Orleans, LA 70112. or Wenxing Hu, Department of Biomedical Engineering, Tulane University. 1440 Canal St, New Orleans, LA 70112.
Helicobacter pylori (H. pylori) infection (HPI) is one of the most widespread diseases. More than half of world population is affected by HPI, especially children in developing countries. The associations between many gastrointestinal diseases and HPI have been found in clinical. Also, there are some diseases whose HPI associations are controversial and unclear. Due to its unclear disease association, H. pylori test is not included in the clinical screening. However, some pre-clinical studies showed possible associations between HPI and these diseases, involving pathological changes of different functional systems of the human body (e.g., Immune system, cerebrovascular system). Therefore, for HPI patients, more attention should be paid to the possible risks of these diseases. In this study, a systematic literature review was conducted to identify and classify H. pylori related diseases. This review identified 175 HPI related diseases belonging to 9 categories, and summarized the corresponding supporting literature reports. In addition, the functional mechanisms underlying the linkages between HPI and 28 well studied diseases were discussed, revealing possible pathogenesis for these diseases. We conclude that HPI is related to many serious diseases affecting multiple important human systems, and clinical HPI treatment and HPI test might help the detection and treatment of these diseases. Our results guarantee further study using more data to testify the possible relations between HPI and these diseases.
H. pylori is a gram-negative and microaerophilic bacterium, usually found in the stomach. Although up to 85 % of people infected with H. pylori never express any symptoms or complications, more than half of world population are infected by H. Pylori [1]. In 1982, H. Pylori was first discovered by two Australian scientists, Barry Marshall and Robin Warren [2]. (reference fontsize) Before that, human gastric ulcers were believed to be caused by stress, spicy foods, smoking, and other malignant habits. Nevertheless, recent epidemiologic and clinical studies have proved that HPI is the main cause for gastric and duodenal diseases. Additionally, HPI has been linked to the pathogenic development of gastric adenocarcinoma [3], the second leading cause of cancer-related death [4].
Acute HPI may appear as an acute gastritis or nausea [5]. Individuals infected with H. pylori have 10 % to 20 % lifetime risk of developing peptic ulcers, and 1 % to 2 % increased risk of developing stomach cancer [6, 7]. The pyloric antrum inflammation leads to duodenal ulcers, while inflammation of the corpus leads to gastric ulcers and gastric carcinoma [8]. A study showed that HPI was related to gastric cancer and the risk of developing gastric cancer was reduced from 1.7 % to 1.1 % with HPI treatment [9].
In addition, H. pylori is also reported to be associated with non-gastrointestinal related disease, including hematological diseases, cardiovascular diseases, and neurological disorders. However, the clinical checks of most of these non-stomachic diseases do not include HPI screening check due to the controversial and unclear HPI association. This review summarizes some previous studies conducted before 2016 exploring possible associations between HIP and other diseases, to identify diseases that could use HPI as their clinical indicators.
We performed a literature search through PubMed, ScienceDirect and Elsevier journal papers. In total, 2,070 articles published from January 1990 to December 2016 were covered, which report potential relations between HPI and some diseases. There were 175 different diseases or symptoms extracted from the literatures, and their detailed information is listed in the Supplementary Data, including the disease name, category, status of association with HPI and the number of supporting references. In this work, we focused our discussion on diseases meeting the following criterions: 1) with no less than 5 papers supporting positive HPI associations; or 2) with at least one paper reporting negative/controversial/no association. Also, these diseases were classified based on the human body system they were related to.
There were 28 different diseases of 9 categories that satisfied the disease selection criteria, which were summarized in Table 1. In total, 1,539 articles (74.3 % of 2070) reported positive associations between digestive-system-related diseases and HPI. Positive HPI affections were also found in atherosclerosis and myocardial ischemia, Alzheimer disease, Parkinson disease, chronic urticarial, and diabetes mellitus. Negative affections were observed in immune response, including asthma, allegic rhinitis, and digestive diseases that are related to peptic acid secretion (e.g., esophagitis, esophageal adenocarcinoma, hyperchlorhydria and inflammatory bowel diseases). Liver cirrhosis, anemia, idiopathic thrombocytopenic purpura, cerebral infarction, hyperemesis gravidarum, and obesity were reported to have controversial HPI associations.
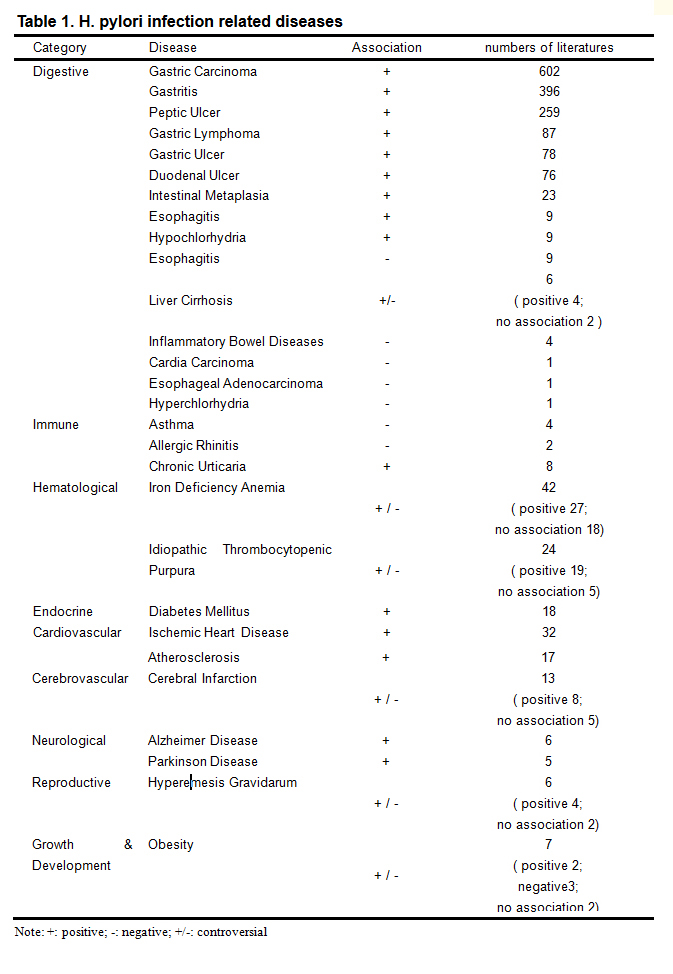 Table 1. H. pylori infection related diseases
Table 1. H. pylori infection related diseases
Note: +: positive; -: negative; +/-: controversial
HPI plays an important role in severe digestive diseases including chronic gastritis, peptic ulcer disease, gastric MALT lymphoma and gastric cancer [10]. HPI was found in 89.8 % of chronic gastritis patients [11]. Fig. 1 shows the gastrointestinal disease progression induced by HPI.
HPI is recognized as a clinical marker for the risk of gastric cancer. It has been shown that HPI could induce gastric cancer through multiple pathogenic steps [12-14]. Chronic gastritis have been demonstrated to be the main cause of gastric MALT lymphoma in HPI patients, and MALT lymphoma induced tumor regression in 70 % to 80 % of patients [15- 17]. Recently, it was found that patients with chronic gastritis caused by HPI have a three times greater risk of developing gastric cancer compared with control groups without HPI [18].
HPI causes chronic gastritis with a mucosal infiltration caused by inflammatory cells [19]. In most cases HPI patients remain asymptomatic for a long time [20]. Due to the fact that H. pylori is covered by the mucous layer, it is hard for the immune systems to eliminate the bacterium colonized at the epithelial cells of the stomach [21]. Chronic HPI could lead to gastric damage associated with digestive problems, and it is dependent on both host and bacterial factors, which is different from many other infections [22-23].
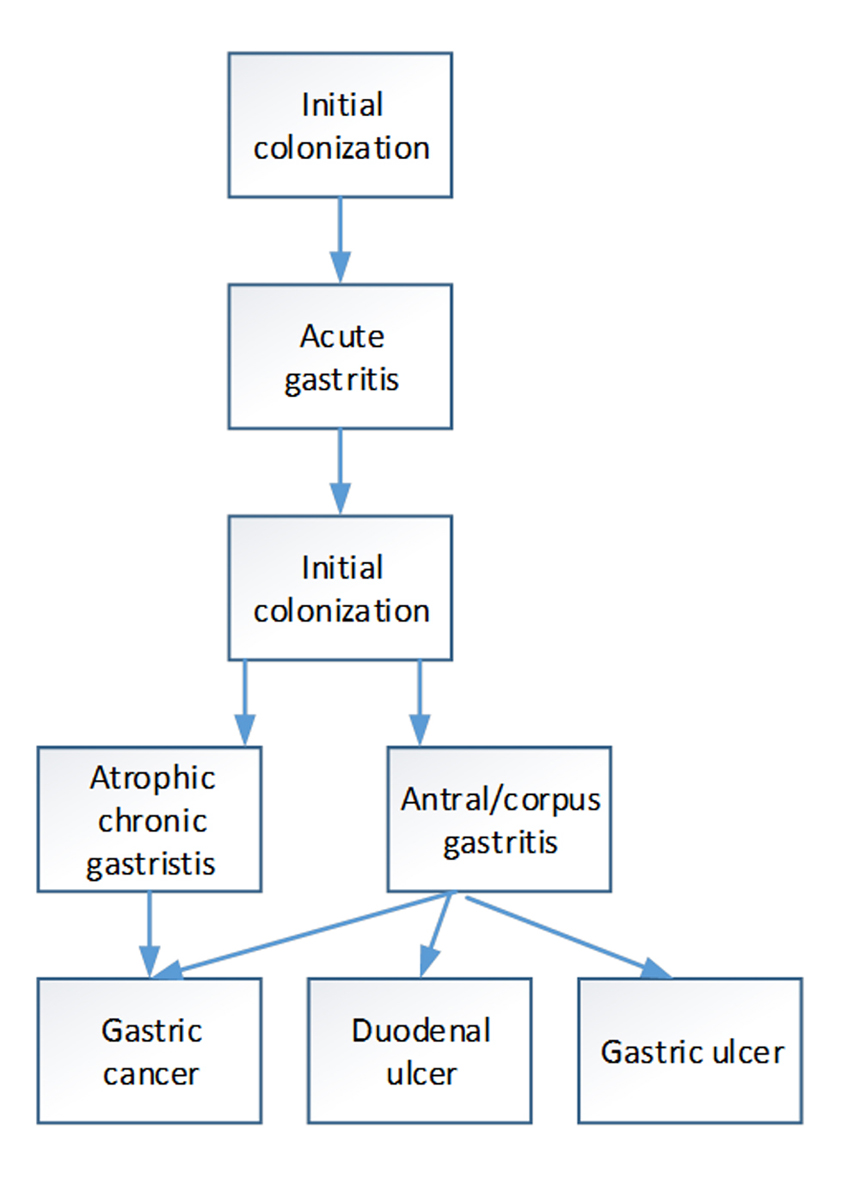 Fig. 1 The H. pylori induced gastrointestinal diseases
Fig. 1 The H. pylori induced gastrointestinal diseases
HPI has been reported to have a negative association with hyperchlorhydria [24], eosinophilic oesophagitis [25] and reflux esophagitis after esophagectomy [26, 27]. In most cases, acute HPI reduces stomach acid secretion at the beginning. The reduced stomach acid secretion usually returns to the normal level after a few months. HPI induces atrophic in the mucosa, leading to persistent hypochlorhydria caused by secretory tissue atrophic. In the early period of esophagogastrostomy, bile reflux could cause reflux esophagitis that is related to HPI [26,27]. The results from Arnim et al.’s study showed that the control group presented significantly higher seroprevalence of H. pylori compared to that of patients with esophagitis [25]. Nishimura et al. reported that the level of gastric acidity in patients with HPI, were significantly lower than that in patients without HPI [26].
Some studies suggested that Cirrhosis was positively associated with HPI. However, other studies did not observe significant relations between HPI and Cirrhosis. A recent meta-analysis [27] showed a significant difference of cirrhosis rates between HPI patients and healthy controls [odd ratio (OR) = 2.05, 95 % confidence interval (CI): 1.3-3.18, p < 0.0001]. However, no significant difference were found in the studies using Asian subjects (OR = 0.90, 95 % CI: 0.48-1.66, p < 0.0001 ) [28]. These conflicting results may be caused by the geographic and race difference of the participants.
3.2 Hematological diseasesIron deficiency anemia (IDA) has controversial HPI association reports. IDA may be induced by HPI [29-32]. Gastrointestinal diseases linked to HPI may cause the inadequate iron intake or chronic blood loss. Dufour et al. were the first to indicate the relation between IDA and H. pylori [29] which was supported by a lower ferritin level in HPI patients [30-32]. Chronic blood loss may be caused by ulcer. The other possible IDA pathogenesis may include the impaired iron absorption caused by atrophic gastritis [33,34]. However, there were some studies supporting negative associations between HPI and IDA [35,36].
The results on the association between HPI and idiopathic thrombocytopenic purpura (ITP) were also controversial. Some studies showed a prevalence of HPI patients with ITP [37-39]. However, these studies have no control groups. Campuzano-Maya presented a higher prevalence of ITP in patients with HPI than the control group [40]. On the contrary, Michel et al. did not find any significant difference in ITP prevalence between the HPI group and the control group [41].
3.3 Cardiovascular diseasesIt has been suggested that H. pylori plays an important role in ischemic heart disease (IHD). HPI may induce deficiency of folate and vitamins. Thereby, HPI might be involved in coronary heart disease pathogenesis [42]. However, some studies have reported conflicting results [43-46]. There may be false positives in IHD patients, which is more related to age and social status [46]. Danesh et al. conducted a meta-analysis and observed no significant positive association between H. pylori and CHD [47]. Some studies reported that more serious coronary atherosclerosis was observed in patients with H. pylori CagA+ strains infection [48-50].
3.4 Cerebrovascular disordersThe potential HPI associations of ischemic atherosclerotic stroke and vascular dementia have also been proposed. Sawayama et al. suggested that chronic HPI may increase the risk of acute ischemic stroke. Their study results showed that chronic H. pylori infection was related to a higher risk of stroke caused by small artery occlusion (odds ratio: 9.68; 95 % CI: 3.56-33.08, p < 0.001), but a lower risk of cardioembolic stroke (odds ratio: 0.27; 95 % CI: 0.03-1.53), and an overall association with ischemic stroke (odds ratio for all subtypes combined: 2.57; 95 % CI: 1.09-6.08) after adjusting major cardiovascular risk factors [51]. However, there were conflicting results on the relevance of chronic infection by H. pylori as a risk factor for ischemic stroke. For instance, a case-control study by Yang et al. failed to identify any strong association between chronic HPI and ischemic stroke [52]. Additionally, the meta-analysis by Yu et al. indicated no significant association between HPI and ischemic stroke [53].
The proposed mechanism linking H. pylori to ischemic stroke is similar to that of IHD. CagA+ strains had been shown to increase the risk of ischemic stroke by affecting the instability of carotid plaque [54-59]. Cross-reacting antibody is a risk factor for carotid atherosclerosis [60]. An alternative explanation for the relationship between cerebrovascular disease and HPI was the hyperhomocysteinemia [61], although it was not confirmed by Markus and Mendall [62].
3.5 Neurological disordersHPI is one of the infections which have been implicated as risk factors for cognitive impairment, dementia and Alzheimer's disease (AD) [63-64]. Kountouras et al. demonstrated a significantly higher prevalence of HPI [65] and anti-H. pylori specific IgG in the cerebrospinal fluid of patients with AD [66].
H. pylori may also trigger Pakinson disease. The eradication of H. pylori could change the course of idiopathic parkinsonism [67] and improve the pharmacokinetic and clinical response to L-dopa in patients with idiopathic parkinsonism by increasing the L-dopa absorption [68]. Schulz et al. supported this theory and stated that cholesterol glucosides may be raised by HPI [69].
3.6 Immune responseNegative HPI associations have been reported with several allergic diseases including atopy, asthma and allergic rhinitis [70-72]. Evidence from epidemiological studies suggested HPI accounted for an estimated 18 % reduction in odds of atopy [70]. Sheptulin et al. suggested a negative HPI association in bronchial asthma and chronic inflammatory intestinal diseases [71]. Reibman also proposed a hypothesis that colonization with CagA+ H. pylori strains had a negative association with asthma [72]. Experimental by Arnold et al. suggested that HPI could exerted a beneficial effect in mouse with asthma [73].
3.7 Diabetes mellitusH. pylori infection is reported to be associated with insulin resistance, diabetes mellitus and metabolic syndrome [74-76]. Compared to non-diabetics with HPI, the levels of oxidative DNA damage (8-OHdG) in type 2 diabetes mellitus could be much higher (p = 0.001). In addition, 8-OHdG levels of these HPI non-diabetics were also higher than that of type 2 diabetes mellitus with negative H. pylori. These results showed a pathogenic linkage between HPI and diabetes [74]. There were significant differences of fasting blood glucose, high-density lipoprotein cholesterol between HPI patients and healthy controls [75]. Hsieh et al. reported that long-term HPI was significantly associated with increased levels of HbA1c and decreased insulin secretion in Chinese population [76].
3.8 Hyperemesis gravidarumH. pylori infection may cause hyperemesis gravidarum (HG). Serologically positive HPI was detected in 44 out of 54 patients with hyperemesis gravidarum (81.5 %) whereas 29 out of 53 asymptomatic gravidas (54.7 %) had positive antibody titers for Helicobacter pylori, and the ratio of Helicobacter pylori seropositivity in pregnant women with hyperemesis gravidarum was significantly higher than that of asymptomatic pregnant women (p < 0.01) [77]. This positive association was also confirmed in several other studies [78,79]. However, some conflicting results were also identified in some other studies [80-81], making the HPI-HG relation more complicated.
3.9 ObesityIt was reported that the association between HPI and obesity could be both positive [82-83] and negative [84-85]. For example, leptin and ghrelin are important appetite hormones secreted from the stomach. They play important roles in the coordination of eating behavior and weight regulation. It was found that the eradication of H. pylori was associated with a significant increase in leptin levels and body mass index (BMI) in pre-pubertal children with H. pylori-associated gastritis [86]. Azuma et al. demonstrated that H. pylori eradication could increase BMI [87]. Nweneka and Prentice presented a systematic review and found that 17 studies showed lower circulating ghrelin levels in H. pylori-positive patients while 10 studies reported no difference, and the meta-analysis of 19 studies involving 1,801 patients showed a significantly higher circulating ghrelin concentration in H. pylori-negative individuals, but H. pylori eradication did not alter the ghrelin levels [88].
HPI is one of the most widespread diseases worldwide, and has been reported to be associated with many diseases affecting multiple functional systems of human body. In this paper, we conducted a systematical literature review in order to detect diseases that have clear and confirmed HPI associations. Clinical and epidemiological cases in some studies showed strong evidences of positive H. pylori associations in some diseases, especially some gastrointestinal diseases, e.g. gastritis and gastric carcinoma, gastric lymphoma. In contrast, H. pylori association patterns in several diseases from some other human systems remains unclear with controversial conclusions. One possible reason is that H. pylori test is not a routine test for non-gastrointestinal diseases. More data are needed in order to test the role that HPI plays in the pathogenesis of these non-gastrointestinal diseases.
Authors claim no conflict of interests.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
68.
69.
70.
71.
72.
73.
74.
75.
76.
77.
78.
79.
80.
81.
82.
83.
84.
85.
86.
87.
88.
Supplementary File 1: Excel File
Li S, Liu M, Garcia E, Hu W. Helicobacter Pylori Infection Associated Diseases – A Systematic Review. Med One. 2017 Apr 25; 2: e170007. https://doi.org/10.20900/mo.20170007

Copyright © 2020 Hapres Co., Ltd. Privacy Policy | Terms and Conditions




