Location:Home >> Detail
Med One. 2018; 3: e180014. https://doi.org/10.20900/mo.20180014

1 Department of Medical Surgical Sciences and Biotechnologies, “La Sapienza” University of Rome, Latina 04100, Italy;
2 Centro Di Riferimento Oncologico-National Cancer Center, Experimental & Clinical Pharmacology, Aviano 33081, Italy;
3 Medical Oncology and Anatomic Pathology Unit, San Filippo Neri Hospital, Rome 00135, Italy.
* Corresponding Author: Francesco Angelini.
This article belongs to the Virtual Special Issue "Application of Stem Cells and Biomaterials in Tissue Regeneration"
Despite several improvements in term of diagnosis and prevention, ischemic heart disease still represents one of the principal worldwide causes of death. Cardiac progenitor cells (CPCs) based therapy is considered a valid alternative to heart transplant, but several issues concerning the transplanted cells viability, retention and therapeutic effect need to be solved. Tissue engineering, mixing synthetic or natural polymers with injected cells, could represent the way through which overcomes shortages and set up an effective cardiac regenerative therapy. Nowadays, it is well known that cardiac extracellular matrix (ECM) provides structural and functional integrity, affects cardiac function, development and physiologic repair. In this optic, ECM and ECM-like materials represent functional and biocompatible tools with a great potential to serve as natural or nature-mimicking scaffolds in the field of regenerative medicine. The aim of the present work is to provide an overview on the state of the art and recent advantages on CPCs and scaffold-based therapy for heart regeneration.
Despite considerable achievements in term of early diagnosis and prevention, ischemic heart disease still represents the leading cause of death and disability worldwide and its frequency is increasing. In 2018, it has been established that ischemic heart disease accounts for almost 1.8 million annual deaths [1]. Nowadays, heart transplantation represents the only successful therapeutic approach for end-stage heart failure (HF) patients. Unfortunately, organ availability and immunological issues heavily hinder this strategy. The need to establish effective therapies, to improve survival and quality of life of the patients, has led researchers to investigate and develop alternative therapies able to protect, regenerate and functionally restore the damaged myocardium. The mammalian heart has been considered, for a long time, as a terminally differentiated organ incapable of regenerating after injury. In recent years, many evidences demonstrated that cardiomyocytes, during aging and after injury, are able to reentry in the cell cycle and promote cell renewal [2,3]. In addition, it has been identified the presence of several resident cardiac progenitor cells (CPCs) population that, after myocardial infarction (MI), are able to proliferate and differentiate into the cardiac lineages [4]. Unfortunately, inflammatory processes following cardiac injury, in addition to the unsuitable ischemic microenvironment and the lack of oxygen, are able to affect this endogenous regenerative process exacerbating tissue damages and promoting adverse remodeling. Accordingly, cardiac cell therapy (CCT) approach, based on isolation, expansion and injection of CPCs, might be a valid alternative to promote and support heart regeneration [5,6]. However, despite the encouraging preclinical and clinical results, these treatments have shown very limited improvement in the long term [7–9]. In fact, it has been demonstrated that many injected cells are lost within few hours after injection and only the 5–10% can be detected after one day in the damaged myocardium [10,11]. The limited engraftment and the subsequent reduced proliferation and differentiation potential of the transplanted cells, due to the interaction between injected CPCs, extracellular matrix (ECM) components and the local tissue condition, represent another important issue for the therapeutic outcome [10,11]. Therefore, the synergy between CCT and tissue-engineering approaches, able to increase the engraftment and regenerative potential of injected cells, in addition to their anti-remodeling capacities and the possibility to stimulate resident cells, could represent a beneficial and valid alternative [12]. In the present review, we discuss the therapeutic role of CPC population and provide an overview on the state of the art and recent advantages on scaffold-based therapy for infarcted myocardium in order to understand which step will be the next to be taken to improve cardiac regenerative medicine.
ECM is a key functional tissue structure, including growth factors, fibrous proteins and glycosaminoglycans (GAGs) produced and secreted by resident cells, able to create an in vivo specialized microenvironment in which cells survival and biological activity is preserved [13]. In the heart, ECM provides structural and functional integrity, mediating the mechanical connection among cardiomyocytes, cardiac fibroblasts (CFs) and blood vessels, able to guide organ development and physiologic repair and to affect cardiac functions [14–16]. CFs, that together with endothelial cells represent the higher portion of resident non-myocyte cells, are able to produce ECM and, at the same time, maintain its homeostasis, through the production of matrix metalloproteinases (MMPs), a group of ECM-degrading enzymes able to break down all the protein components of the matrix, and the tissue inhibitors of metalloproteinases (TIMPs) [17,18]. Several pre-clinical and clinical studies have underlined that an imbalance in ECM remodelling, which means an alteration between the MMPs and TIMPs production and function, is detrimental in the failing heart [19–23]. In fact, this maladaptive remodelling, bringing to an altered arrangement and reduced cross-linking between collagen fibres, contributes to reduce systolic performance, decreased compliance and diastolic dysfunction in failing human heart [24]. Furthermore, inflammatory cytokines such as interleukin-1b (IL1b), interleukin-6 (IL6) and tumor necrosis factor-α (TNFα) can promote the differentiation of CFs into collagen-producing myofibroblasts, increasing the relative amount of the stiffer collagen type I over the more compliant collagen type III [25–27]. The increase in myocardial stiffness, from a physiologic 10–20 kPa Young’s Modulus to a 50–200 kPa range, leads to an autocrine feedback signalling able to support a mechanically induced fibrosis that ends up in chronic scarring process [28]. Furthermore, it has been demonstrated that during this cardiac adverse remodeling, variations in ECM composition and its mechanical features can interfere with the cardiogenic potential of resident or transplanted CPCs [29]. In this optic, ECM and ECM-like materials represent functional and biocompatible tools with a great potential to serve as natural or nature-mimicking scaffolds in the field of regenerative medicine [30,31].
The heart has been considered for a long time as a terminally differentiated organ with no intrinsic capacity to regenerate after myocardial injury. This concept is now being challenged and several evidences demonstrated that into the adult mammalian heart, both in normal and pathological conditions, myocytes are able to undergo mitosis and cytokinesis [32]. Furthermore, different resident cardiac progenitor cells (CPCs) populations have been identified both in the embryonic and adult heart and their potential use for cardiac regeneration has been deeply investigated for years [33].
3.1 Embryonic CPCsDuring the embryonic development, multipotent cardiovascular progenitors (MCPs), which derive from the mesodermal lineage, contribute to the heart formation in two ways [34]. On one side, the First Heart Field (FHF), which is the classical cardiac crescent consisting of T-Box 5 (TBX5) positive cells, is known to contribute to the formation of the left ventricle and, partially, of the atria. From the other side, the Second Heart Field (SHF), mainly composed of LIM-homeobox Transcription Factor Islet-1 (ISL1) positive cells, contributes to the formation of the right ventricle, the outflow tract and the remaining parts of the atria [35,36]. Due to their ability to differentiate into cardiac and smooth muscle and vascular endothelium, MCPs represent a promising regenerative tool for heart repair [37,38]. In fact, embryonic stem cells (ESCs) have been deeply studied not only to investigate cardiac development and the function of human and murine heart cells, but also to determine the basic strategies of regenerative cell therapy [39–41]. Furthermore, several in vitro protocols have been developed to stimulate human ESCs differentiation in cardiomyocytes, providing a morphology and an expression profile similar to that of adult cardiomyocytes [42]. Briefly, cardiomyocytes markers are categorized in two principal groups: early and late differentiation. After 5–6 days of differentiation, GATA Binding Protein 4 (GATA-4), Isl1, and Kinase Insert Domain Receptor (KDR) become highly expressed. Later, between 8 and 10 days of differentiation, the expression levels of NK2 homeobox5 (NKX2.5), Tbx5, Myocytes-Specific Enhancer Factor 2C (MEF2C) and HAND1/2 reach an expression peak together with an increase in myofilament-related gene expressions, such as Troponin T2 (Tnnt2) and Myosin Heavy Chain 6 (Myh6) [43]. Nevertheless, despite MCPs high plasticity, their introduction into the clinical trial/therapeutic scenario is affected by several problems, in particular ethical issues, the genetic variability, the risk of immune rejection and the tumorigenic possibility [44].
3.2 Adult CPCsEven if their physiologic role in homeostasis and activation after injury still remains unclear, CPCs can be isolated from adult human and mammalian hearts with different approaches [45–47]. For example, side population cells (SP) are defined by their ability to efflux the DNA-binding dye Hoechst 33342, whereas Sca1+ population is characterized by the expression of the stem cell antigen-1 [48,49]. Interestingly, in 2004 it has been demonstrated for the first time that human CPCs can be isolated, starting from explant cultures of percutaneous endomyocardial biopsy specimens, through their capacity to form spontaneously 3D spherical clusters, called cardiospheres (CSps) [50–53]. CSps represent a perfect niche microenvironment in which it is possible to recognize, according to their expression pattern, two distinct compartments. The core, in which cells are characterized by a high proliferation rate, presents a cardiac progenitor immunophenotype dominated by the expression of stem cell and cardiomyocyte-related antigens, such as c-KIT, GATA-4, NKX2.5, CX43 and OCT4. On the contrary, peripheral cells are characterized by a more committed expression profile into endothelial, mesenchymal, or cardiomyogenic lineages (CD105, MHC, TNI, CD31, CD133, MDR1) [52,54]. CSps can be expanded in monolayer as CSps derived cells (CDCs) to obtain a culture enriched in CPCs, previously selected through the CSps formation step [51]. CDCs are defined by clonal growth capacity and, phenotypically, by several characteristic markers, such as α-SMA, CX43 and CD105 that positively identify more than 80% of CDCs, resulting negative, at the same time, for hematopoietic and endothelial progenitor cell markers [55]. Interestingly, CDCs can acquire a mature cardiomyocyte phenotype when co-cultured with neonatal rat ventricular myocytes (NRVMs) [55]. Although it has been analysed the therapeutic potential of other non-cardiac stem cell sources, such as embryonic cells, bone marrow-derived mesenchymal stem cells, endothelial progenitor cells, myoblasts and induced pluripotent stem cells, many evidences underlined that resident CPCs, especially CDCs, represent the better candidate for cardiac regenerative medicine [5,56–59]. In 2012, Li et al., using a mouse model of myocardial infarction (MI), demonstrated that the functional outcome of CDCs transplantation was superior to the transplantation of bone marrow mesenchymal stromal cells and adipose-derived regenerative cells [58]. Subsequently, other preclinical studies confirmed that CDCs therapy has multiple beneficial effects on the damaged myocardium, such as enhancement of cell survival, increase of blood supply and viable mass, reduction of inflammation and scar size and, in acute MI pig models, prevention of ischemic injury after reperfusion [60–65]. These encouraging preclinical results have paved the way to CDCs-based clinical trials. In 2012, the CADUCEUS study (NCT00893360) investigated the intracoronary administration of autologous CDCs after acute myocardial infarction [66]. In the 6-month follow-up, the safety of the cells was demonstrated in association with a reduction of the infarct scar size and an increase in myocardial viability and contractility [66]. Furthermore, after 1 year from the treatment, even if ventricular volumes and left ventricular ejection fraction (LVEF) did not increase, myocardial regeneration has been achieved, strengthened the therapeutic potential of CDCs [67]. In the same year, another clinical trial started, the ALLSTAR study (NCT01458405), in order to evaluate the effect of allogeneic CDCs on scar size in patients with post-MI ischemic left ventricular dysfunction [68]. Unfortunately, the study is still in progress and results are not yet available. Interestingly, even if CPCs show a high differentiation potential in vitro, recent studies suggest that the in vivo direct differentiation following transplantation is not the primary mechanism by which these cells promote cardiac recovery [6]. In fact, a great proportion of CPCs therapeutic effects were shown to be attributable to indirect mechanisms of action able to exert protective and beneficial effects on the endogenous tissue. In a comparative study, it has been analysed the CPCs secretome profile, consisting of humoral factors, proteins, and molecules, underlining a highly complex and biological activity able to provide significant paracrine benefits than other progenitor populations, such as the bone marrow or adipose tissue [58]. Indeed, CPCs secretome exerts significant anti-apoptotic effects, promotes the recruitment of endogenous progenitors and the activation of endogenous cardioblasts [69–71]. In this context, also CPCs-derived exosomes are able to exert, once released in the extracellular microenvironment, positive therapeutic effects through multiple mechanisms interacting with different target cells, such as endothelial cells and cardiomyocytes [72–74]. Overall, despite all these encouraging results many critical issues, including the challenges of electrical coupling, undetermined mechanism aspects and, above all, the long term engraftment and survival of injected cells, should be addressed before CPCs could be considered as a strong therapeutic tool for regenerative medicine applications [75].
Tissue engineering could be defined as a synergistic cooperation, between biotechnological, biomedical and engineering knowledges and applications, which aims to regenerate damaged tissues and/or organs. In the cardiac regenerative medicine field, one of the most important issues of tissue engineering is the development of functional artificial tissues and organs. The ideal engineered product has to provide an adequate cellular niche microenvironment able to mechanically support and direct cell growth, differentiation and engraftment, protect the transplanted cells from the hostile infarcted tissue environment and, as an outcome, to promote tissue remodeling/regeneration [12,76]. For all those reasons, biocompatibility, biodegradability and permeability represent the unavoidable characteristics that the biomaterial must possess [77].
4.1 Polymers for cardiac tissue engineeringPolymers, characterized by a wide range of compositions and, thus, properties, represent one of the most used classes of biomaterials to recreate EMC-mimicking scaffolds for cardiac regeneration. In general, polymers can be classified in synthetic or natural (Table 1). Briefly, synthetic materials, such as Polyglycolic acid (PGA), polylactic-l-acid (PLLA), polylactic glycolic acid (PLGA) and polyurethane (PU), that are extremely malleable, are not always biodegradable and often prevent vascular and parenchymal cell attachment and infiltration [78,79]. Besides, natural polymers, or biopolymers, such as collagen, elastin, chitosan, cellulose and hyaluronic acid, even if exhibit a higher degree of biocompatibility and promote cell migration and differentiation, present a low mechanical strength for cardiovascular application [80]. Therefore, it has been proposed the combination of synthetic and natural biomaterials to improve the weakness of each polymer to create a scaffold with better properties [79,81]. Nowadays, one of the most promising approaches investigated for cardiac tissue engineering involves the use of bioactive glasses (BGs) [82]. BGs, since their discovery by Hench et al in 1969, have gained much attention in tissue engineering due to their highly biocompatibility and bioactivity and are recognized as the second generation of biomaterials with the ability to bond to the living tissues [83]. Based on their composition, BGs can be categorized as silicate-based glasses, borosilicate and borate-based glasses, and phosphate-based glasses. Recently, BGs has been considered as suitable materials for cardiac tissue engineering, especially in the form of nanoparticles in combination with biocompatible polymers acting as soft matrices [82,84].
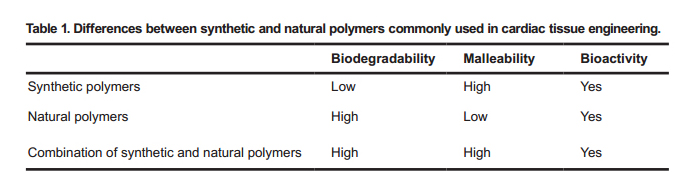 Table 1. Differences between synthetic and natural polymers commonly used in cardiac tissue engineering.
Table 1. Differences between synthetic and natural polymers commonly used in cardiac tissue engineering.
In the last years, many studies investigated the creation of autologous biological scaffolds composed of native ECM, derived from the decellularization of tissues or organs, in order to provide tissue-specific ECM compositions, which can influence the behavior of resident and/or transplanted cells [85,86]. Recently, Seo et al. developed a detergent-free decellularization protocol based on supercritical carbon dioxide and ethanol co-solvent (scCO2-EtOH) method able to prevent ECM structure disruption. They tested this decellularized ECM (dECM) on rat heart tissues, demonstrating that heart-derived dECM with scCO2-EtOH treatment, compared to a collagen control group, represented a promising angiogenic material for healing in ischemic disease [87]. In general, the decellularization process, removing cell components, is able to leave unchanged tissue architecture, ECM components and, thus, mechanical properties [88,89]. In addition, eliminating antigenicity, in case of xenogenic or allogeneic transplant it reduces the possibility of inflammatory and immune responses [90–94]. A variety of non-cardiac tissue types have been tested as decellularized ECM source in order to repair myocardium after an ischemic injury, such as small intestine submucosa or urinary bladder matrix [95–97]. However, it has been demonstrated that cardiac ECM exhibits tissue-specific composition and organization, therefore the utilization of an ECM from non-cardiac tissues may fail to provide proper stimulations to cells in the myocardium [98,99]. Nowadays, pericardial and myocardial tissues represent the principal cardiac-source for ECM [100,101]. The pericardium is a double-walled fibrous sac, primarily composed of collagen and elastin, that contains the heart and the roots of the great vessels, fixing them to the mediastinum, and it is able to confer protection against infections and lubricates the heart [95,102]. Myocardium is the thick contractile middle layer of the heart wall composed of muscle cells. Myocardial ECM is principally composed of a mixture of different collagen types (80% type I, 10% type III, < 5% type V) in addition to a small amount of laminin, elastin and fibronectin [103].
4.3 3D scaffoldsDespite contributions in biomedical research and the development of more complex 2D culture platforms, it is difficult to predict, recapitulate and understand cell-cell interactions and functions, naturally designed for a 3D environment, in a bi-dimensional context. Cardiac ECM, secreted by resident cells, consists of structural and functional three-dimensional molecules-based organization that establish cardiac ultrastructure and microenvironment [104]. In this optic, 3D scaffolds, could represent a perfect physiological and pliable pattern to promote an effective tissue remodelling and regeneration in damaged cardiac tissues, enhancing in resident and/or transplanted CPCs chemotaxis, proliferation and differentiation [105]. In terms of patch architecture many different systems have been investigated and are available for scaffold creation. In 2002, Taylor et al. demonstrated that 3D biodegradable collagen sponge-based scaffold, composed of interconnected micropores, with notable fluid absorption and hydrophilicity, was able to maintain viable human cardiac valve interstitial cells (ICs) and to enhance the capacity of those cells to express their original phenotype, making this scaffold suitable to resemble a valve leaflet [106]. A different approach is based on mesh-based scaffold, in which biomaterial fibers are braided in a 3D structure with uniform porosity and dimensions similar to the ones naturally occurring in the ECM. A comparison of the structural and biological features of a collagen fibrous ball-of-thread-like versus a gelatin trabecular sponge-like bio-constructs, seeded with human CSps, demonstrated that both scaffolds, despite their structure or composition, recreate a more pro-survival and cardiac-specific differentiative microenvironment than the normal in vitro culture protocols [107]. Recently, it has been compared, both in vitro and in vivo, the effect of a biodegradable and non-toxic PU-based scaffold, grafted with laminin-1 (PU-LN1) or gelatin (PU-G), populated with human CPCs [108]. Compared to the PU-G, used as control, PU-LN1 is able to highly promote cells proliferation, protection from apoptosis and expression of differentiation markers for cardiomyocytes, endothelial and smooth muscle cells. Furthermore, once LN1 scaffolds are implanted subcutaneously in a mouse model of MI, they are able to minimize inflammation and, stimulating blood vessel density around them, to perfectly integrate with the host tissue [108]. Similarly, Wang et al. developed, for the first time, a 3D collagen-elastin scaffold, for heart valve engineering, without chemical crosslinker and assembled by temperature-triggered gelling [109]. Whoever the reduced cell toxicity, the novelty of this approach consists in the co-culture of valvular interstitial cells (VICs), encapsulated in the matrix, with valvular endothelial cells (VECs), cultured on the surface of the 3D structure. Thereby, this scaffold was able to stimulate cell proliferation, to increase actin filaments and to improve integrin β1 expression, representing a novel platform to better study and understand, cell-cell or cell-matrix interactions and, possibly, to improve cardiac valve tissue engineering [109]. As said previously, native ECM could represent a suitable mechanical and biological environment able to ensure cell engraftment and to improve therapeutic and regenerative properties of resident and transplanted cells [29,110,111]. Several studies demonstrated the positive effects of cardiac dECM patch in damaged cardiac tissue. In 2016, a porcine cardiac dECM was implanted in acute and 8-weeks chronic MI rat models [112]. In both conditions, dECM was rapidly vascularized and was able to promote an improvement in cardiac function through the recruitment of resident CPCs, their stimulation towards the cardiomyocyte lineage and their arrangement in partially striated and immature muscle fibers [112]. Furthermore, in the last years, even if the debate on the benefits of this method is still in progress, it has been investigated the possibility to combine in vitro cardiac dECM with CPCs and to apply this “cellularized” patch for in vivo treatments [113–115]. In 2014, Rajabi-Zeleti et al. fabricated a 3D macroporous cardiac patch from human decellularized pericardium membranes (dPM) [116]. They demonstrated that the dPM macroporous scaffold is able to enhance the proliferation, viability, migration and differentiation of CPCs in vitro. Furthermore, after an in vivo subcutaneous implantation, besides the improvement in cells differentiation, the dPM scaffold was able to stimulate angiogenesis and to avoid immune rejection [116]. Recently, a 3D macroporous cardiac patch from solubilized myocardium dECM with the addition of chitosan (CS) has been successfully designed and fabricated [110]. The novelty was represented by the possibility, modifying the percentage of solubilized dECM and CS, to modulate the stiffness of the scaffold according to the requirements. CPCs seeded on this malleable microporous myocardium scaffold present a high proliferation rate and viability in addition to a significant increase in expression of early cardiac markers [110]. Taking together, all these results could be give reasons to investigate and to elucidate how fabricated scaffold could be used to stimulate CPCs differentiation into cardiomyocytes, aiming to create the perfect dECM-derived cardiac regenerative patch.
4.4 HydrogelsOne of the principal aim of cardiac regeneration is to repair ischemic tissues, stimulating the formation of new blood vessels, through the delivery of angiogenic growth factors, stem cells or expansion of pre-existing cells. Despite the encouraging results previously analyzed, one of the problem associated with the use of 3D patch for cardiac repair is the lack of a complete vascularization able to affect the thickness of the scaffold and, as a consequence, cells viability [117]. Furthermore, the necessity to develop minimally invasive techniques requires the setting up of alternatives. In this optic, injectable hydrogels represent the most investigated biomaterials forms for both in vitro and in vivo cardiac tissue engineering (Table 2) [118,119]. Hydrogels can be defined as viscoelastic system, composed of a natural or synthetic extensive water-swollen polymeric network, that can be injected in liquid state and then able to form a solid gel in situ [120]. In 2004, Christman et al. investigated, for the first time, the effects of an injectable biopolymeric fibrin scaffold to deliver cells directly into the infarct wall of MI model rats [121]. Their rationale was that the direct injection in the infarcted myocardium of cells, in this case skeletal myoblasts, would increase cell transplant retention and survival within the infarct. Even if fibrin glue was not able to increase cells retention, the injection of this hydrogel was able to promote cells survival and blood supply to the ischemic myocardium leading to a reduction of infarct size and myocardial remodeling [121]. In addition, the same group demonstrated that an injectable porcine ventricular ECM-derived hydrogel was able to promote in vitro proliferation, survival and cardiogenic potential of embedded human Sca1+ CPCs population [122]. The subsequent injection of the hydrogel in an induced MI rat model resulted in a reduced cardiomyocyte apoptosis, cardiac hypertrophy and fibrosis. On the other side, the resulted increase in resident CPCs recruitment, in cardiac transcription factor expressions and in the neovascularization of the infarcted tissue, has led to an improvement in global cardiac functions and hemodynamics [123–125]. These results in accordance with the needed to provide increasingly effective therapeutic tools have triggered a still ongoing clinical trial (NCT02305602) that evaluates the safety and feasibility of the porcine myocardial dECM-derived hydrogel delivered, in a minimally-invasive procedure, via catheter to the damaged cardiac tissue in patients after myocardial infarction [125–127]. It has been deeply demonstrated that human cardiac dECM-derived hydrogels support in vitro proliferation and differentiation of pluripotent stem cells along the cardiomyocyte lineage in addition to a cytoprotective effect [128,129]. Nonetheless, the porcine dECM application is favoured than human one because of the rarity of collecting healthy human hearts, the significant patient-to-patient variability and, most of all, the aging-related alteration in ECM composition [27,130,131]. Either way, other clinical trials have been developed to investigate the in vivo therapeutic efficacy, safety and feasibility of other hydrogel compositions [126,132]. For example, the PRESERVATION-1 trial (NCT01226563) evaluated the safety and effectiveness of an alginate hydrogel, intracoronary injected, for the prevention of ventricular remodeling and congestive heart failure after MI [133,134]. Furthermore, despite the hydrogel composition, the suitable injection site represents another issue to be investigated. In a recent study by Garcia et al., it has been tested on a pig model of atrial fibrillation (AF) the efficacy of amiodarone, an effective lipophilic medication approved for rhythm control but with a significant systemic toxicity, encapsulated in a PEG-based hydrogel (50 mg amiodarone/5 mL gel) and injected directly on the atrial pericardium. They demonstrated that pericardium hydrogels can deliver therapeutics directly to the heart enabling a continued release of drug for several weeks and reducing off-target organ accumulations [135]. These results highlight the possibility to use pericardium as an alternative therapeutic site for treatment strategy for AF and other cardiovascular diseases. Interestingly, Zhang et al., aimed to test in vitro the efficacy of the pretreatment with pericardial fluid (PF) from rats with myocardial infarction (PFMI) on CSps and to assess, for the first time, the therapeutic in vivo effect on rat models of MI by administering these pretreated CSps, embedded in a commercial hydrogel, in the pericardial cavity [136]. in vitro experiments demonstrated that PFMI pretreatment enhanced CSps survival and their commitment in cardiac muscle cells. Interestingly, the in vivo pericardial application of hydrogel with functionally enhanced CSps demonstrated that these cells could differentiate in cardiac myocytes and, in a paracrine way, to improve cardiac function and myocytes survival, to stimulate angiogenesis into the infarcted myocardium and to reduce myocardial fibrosis [136].
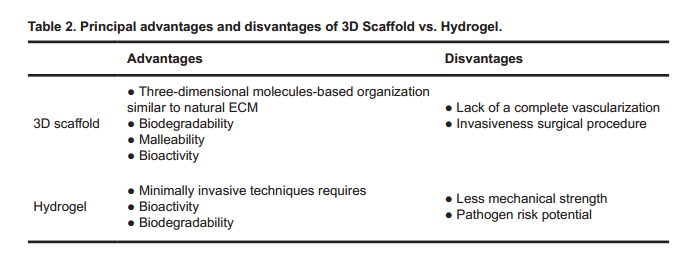 Table 2. Principal advantages and disvantages of 3D Scaffold vs. Hydrogel.
Table 2. Principal advantages and disvantages of 3D Scaffold vs. Hydrogel.
Bioprinting technique, earlier called cytoscribing, represents the last frontier in cardiac tissue engineering and could be defined as computer-aided additive biofabrication of 3D cellular tissue constructs [137–139]. This quickly progressing automated technology allows to strictly controlling the micro and macro-architecture of replacement tissues and organs providing high reproducibility and precise control [140]. Up to date, many tissue types, such as bone, vasculature, neural tissue and cardiac muscle, have been created starting from autologous and patient specific primary or stem cells [141–143]. The basic unit of the entire printing process is the so-called “bioink” that has to be biocompatible and stable from a mechanical and structural point of view [144,145]. Generally, the printable material is composed by living cells, such as embryonic, adult, or induced pluripotent stem cells, proteins and other active biological molecules loaded into a matrix, mimicking the ECM. According to their base materials, bioinks could be divided in two principal groups: scaffold-based and scaffold-free bioinks (Table 3) [139,146–148]. In the first group, cells are seeded within natural or synthetic hydrogels, such as collagen, fibrin and polyethylene glycol, or in dECM [146,149]. On the other side, cells in the scaffold-free bioinks are printed without matrix support and the ability to deposit their own ECM is exploited to confer support for cell-cell communication and proliferation to create strands or spheroids [147,148]. Despite the selected bioink, up-to-date three different bioprinting processes are available [150]. The technical gold standards are represented by viability, spreading and proliferation of cells, in addition to the functionality of the bioprinted constructs [151]. Droplet-based bioprinting (DBB), based on a two-dimensional inkjet printing, was the first developed and it is still the most commonly used methodology. Even if DBB is cost-effective and allows obtaining an 85% of bioink-cell viability, the lower resolution, due to the wide-range of drop size (50–300 µm), represents an important technical limitation [152,153]. In the Extrusion-based bioprinting (EBB), bioink is deposited in cylindrical lines, instead of droplets, by a controlled fluidic dispensing system. EBB offers a great flexibility in printing a wide range of bioinks, such as spheroids or tissue strands, with a considerable print speed, encouraging scalability and clinical translation. However, from a practical point of view, the resolution of printed features is still very low and the percentage of cell viability is around the 80% [153,154]. Finally, in the Laser-based bioprinting (LBB), also known as Stereolithography-based bioprinting (SBB), a laser pulse induces the bioink to acquire a drop shape in order to form 3D constructs. Throughout this artifice, it is possible to obtain a higher precision and resolution, mechanical stress is reduced and cell viability stands around the 95% [153]. Unfortunately, at least for the moment, the high costs and the complexity of the laser system make this technology not easily accessible. From a practical point of view, currently bioprinting research for cardiovascular tissue regeneration largely focuses on the myocardium, heart valves, and vasculature [150]. For example, Gaetani et al. evaluated the therapeutic potential of a 3D-printed patch composed of human Sca1+ progenitor cells in a hyaluronic acid/gelatin (HA/gel) based matrix, transplanted in a mouse model of MI. They observed that the application of the patch led to a significant reduction in adverse remodeling and preservation of cardiac performance. Furthermore, the matrix supported the long-term in vivo survival and engraftment of CPCs, which exhibited a temporal increase in cardiac and vascular differentiation markers over the course of the 4 week follow-up period. Overall, they developed an effective and translational approach to enhance CPCs delivery and action in the heart [155]. Wang et al. have recently provided another example of the feasibility of bioprinting in achieving functional cardiac tissues [156]. They integrated isolated neonatal rat ventricular cardiomyocytes in a composite hydrogels preparation and dispensed this bio-mixture to form a string form or patch form. Interestingly, after 1 week in culture, they observed a spontaneous and synchronous beating of bioprinted cardiac tissues and, in parallel, the formation of dense and uniformly aligned heart muscle bundles. Differently, Ong et al. proposed a culture protocol for 3D bioprinting of cardiac tissue without the use of biomaterials [157]. Firstly, they co-cultured isolated cardiomyocytes, endothelial cells and fibroblasts in low attachment 96-well plates leading to the formation of spontaneous beating spheroids. The possibility to create different mixtures, which differ in term of cell type’s percentage, allows obtaining, depending on the purpose, many different types of printed cardiac patches, with distinctive histological and mechanical properties. Furthermore, the innovative feature of this protocol was the possibility to pick up individual spheroids using vacuum suction and position them on a needle array. Accordingly, spheroids could be precisely positioned in any desired configuration and fused together to create a scaffold-free functional 3D bioprinted patch with mechanical integration of component spheroids. As said previously, bioprinting has been explored also for cardiac valve construction in order to enhance physiological characteristics, such as durability or anticoagulation, compared to traditional mechanical and biological prosthesis valve replacements [158]. Therefore, many evidences, underlined how, through bioprinting approaches, it is possible to obtain a better ECM deposition, an upregulation of muscle actin and a strong human aortic valvular interstitial cells (HAVICs) phenotype [150,159,160]. To summarize, compared to traditional therapeutic strategies, 3D bioprinting may offer a unique approach for creating complicated cardiovascular implants with biomimetic features, which are capable of recapitulating both the native physiochemical and biomechanical characteristics of the cardiovascular system. Furthermore, the current implementation of this technique with the latest pre-vascularization technologies will lead to the improvement of blood perfusion throughout the engineered tissue. For this reason, in the near future, it will be implemented a physiological mimicry of human cardiovascular tissues in order to be applied for an effective drug development, therapeutic approaches and, through the reconstruction of fully functional organ, to overcome the shortage of organ transplantation [150,161,162].
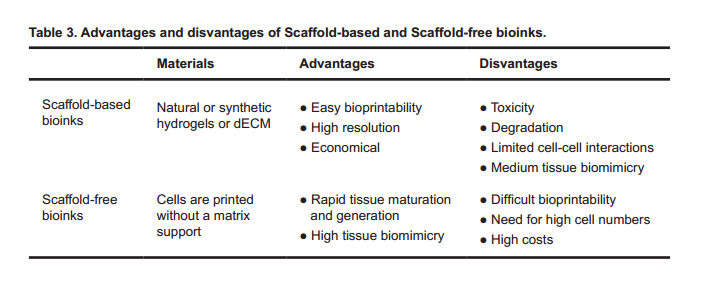 Table 3. Advantages and disvantages of Scaffold-based and Scaffold-free bioinks.
Table 3. Advantages and disvantages of Scaffold-based and Scaffold-free bioinks.
Enormous progress has been made, in the last decades, in cardiac tissue engineering, rendering the clinical application of biomaterials increasingly plausible. However, the concepts discussed in the present review represent just a portion of the great amount of investigations that are still ongoing to insert cardiac tissue engineering in the clinical routine. Actually, the complexity of the heart system, not only because of its mechanical and structural function but also due to its electrical properties as well, still need many efforts to implement our knowledge of the entire panel of variables that influence its regeneration and repair mechanisms. For these reasons, it would be desirable, in the near future, to support scientific cooperation in order to build consensus in all the aspects underlined here, starting from the detection of the best material to the suitable scaffold production technique, without overlooking the selection of the powerful cellular therapeutic tool. In fact, only in this way many issues could be solved boosting cardiac tissue engineering as an effective therapeutic choice for millions of heart patients.
The authors declare that there is no conflict of interest regarding the publication of this paper.
F.A. was in charge of overall direction and planning. F.A and V.P. devised the main conceptual ideas and proof outline. V.P., T.D.R. and F.A. wrote the manuscript.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
68.
69.
70.
71.
72.
73.
74.
75.
76.
77.
78.
79.
80.
81.
82.
83.
84.
85.
86.
87.
88.
89.
90.
91.
92.
93.
94.
95.
96.
97.
98.
99.
100.
101.
102.
103.
104.
105.
106.
107.
108.
109.
110.
111.
112.
113.
114.
115.
116.
117.
118.
119.
120.
121.
122.
123.
124.
125.
126.
127.
128.
129.
130.
131.
132.
133.
134.
135.
136.
137.
138.
139.
140.
141.
142.
143.
144.
145.
146.
147.
148.
149.
150.
151.
152.
153.
154.
155.
156.
157.
158.
159.
160.
161.
162.
Picchio V, Di Raimo T, Angelini F. CPCs and ECM: A Good Mix for Cardiac Regeneration. Med One. 2018 Dec 27; 3: e180014. https://doi.org/10.20900/mo.20180014

Copyright © 2020 Hapres Co., Ltd. Privacy Policy | Terms and Conditions




