Location:Home >> Detail
Med One. 2018; 3: e180005. https://doi.org/10.20900/mo.20180005
 ,
Marinônio Lopes Cornélio 3
,
Marinônio Lopes Cornélio 3
1 Domingo Braile Institute of Sao Jose do Rio Preto, Rua Luiz Vaz de Camoes, 3111 - Vila Redentora, Sao Jose do Rio Preto - SP, 15015-750, Brazil;
2 Associação Brasileira de Nutrologia (ABRAN)/Brazilian Association of Nutrology, Rua Belo Horizonte, 909-Centro, Catanduva - SP, 15801-150, Brazil;
3 São Paulo State University (Unesp), Institute of Biosciences, Humanities and Exact Sciences (Ibilce), Campus São José do Rio Preto, São José do Rio Preto - SP, 15054-000, Brazil.
*Corresponding Author: Idiberto José Zotarelli Filho.
Background: Spontaneous coronary artery dissection (SCAD) may predict fibromuscular dysplasia (FD) in lean Caucasian women, aged 15–50, with no prior history. There is a marked predominance in females with 75.0 to 100.0% of the cases.
Objective: This study undertook a meta-analysis of matrix metalloproteinases 2 and 9 actions and inhibitions in the context of fibromuscular dysplasia and subsequent spontaneous coronary artery dissection.
Methods: The literary search criteria used the Mesh Terms cited in the "Search strategies" section. One hundred and four papers submitted for eligibility analysis were collated, twenty-six studies were selected. The review protocol was based on the criteria of literary search with the use of mesh terms in the main databases such as Pubmed, Medline, Bireme, EBSCO, and Scielo.
Conclusion: The patient was diagnosed with this pathology based on a prior acute myocardial infarction and the presence of coronary tortuosity which are SCAD predictors. Post-treatment as described below, the patient remained asymptomatic.
Spontaneous coronary artery dissection (SCAD) may be a predictor of fibromuscular dysplasia (FD) [1,2] affecting lean, Caucasian women, aged 15–50, with no history [3]. There is a marked predominance in females who constituted 75.0 to 100.0% of all cases. The average age being 30–55 [3]. Some studies have also identified this lesion in older postmenopausal women [4–6].
SCAD is a non-traumatic event generated by coronary artery wall segmentation which creates a false lumen [1,2,7]. It infrequently causes acute coronary syndrome (unstable angina) and sudden death. Its pathological mechanism is poorly understood. SCAD is only known to associate with the vascular system, inflammatory processes, and vasculopathies, with fibromuscular dysplasia (FD) being the primary main one. Arterial and vein tortuosity being the main morphological sign [2].
FD pathogenesis of can result from elastic fiber fragmentation resulting from degrading by matrix metalloproteinases 2 and 9 (MMP2, MMP9) [7]. The MMP roles and inhibitors in FD pathogenesis remains unexplored. More clinical studies are needed to better understand the relationships of these enzymes and how coronary and other vessels are involved [7,8] .
The main predictors of this enzymatic breakdown are postpartum, multiparity, tissue disorder, hormone therapies (use of contraception), certain illicit drugs, physical, and emotional, stress. To a lesser degree it associates with syndromes such as Marfan, Ehlers-Danlos, and Horner [9–12].
The MMP pathophysiological control mechanism is unclear. Any decision to treat SCAD invasively, or non-invasively, follows an analysis of clinical and angiographic factors including dissection site, number of vessels affected, and hemodynamics [3]. Coronary angioplasty with stent implantation may restore flow, alleviate symptoms, and treat dissection. It has a 65% success rate. Coronary artery bypass surgery is reserved for multivessel SCAD and trunk dissection. There are no studies evaluating long-term drug treatment [3].
The present study meta-analyzed the action and inhibition of matrix metalloproteinases 2 and 9 in the context of fibromuscular dysplasia and subsequent spontaneous coronary artery dissection.
One hundred and four papers were collated after being selected by using as the literature search criteria the “Mesh Terms” identified in "Search Strategies". Twenty-six studies were examined following the rules of systematic review-PRISMA (Transparent reporting of systematic reviews and meta-analyzes: http: //www.prisma-statement.org/), as shown in Fig. 1
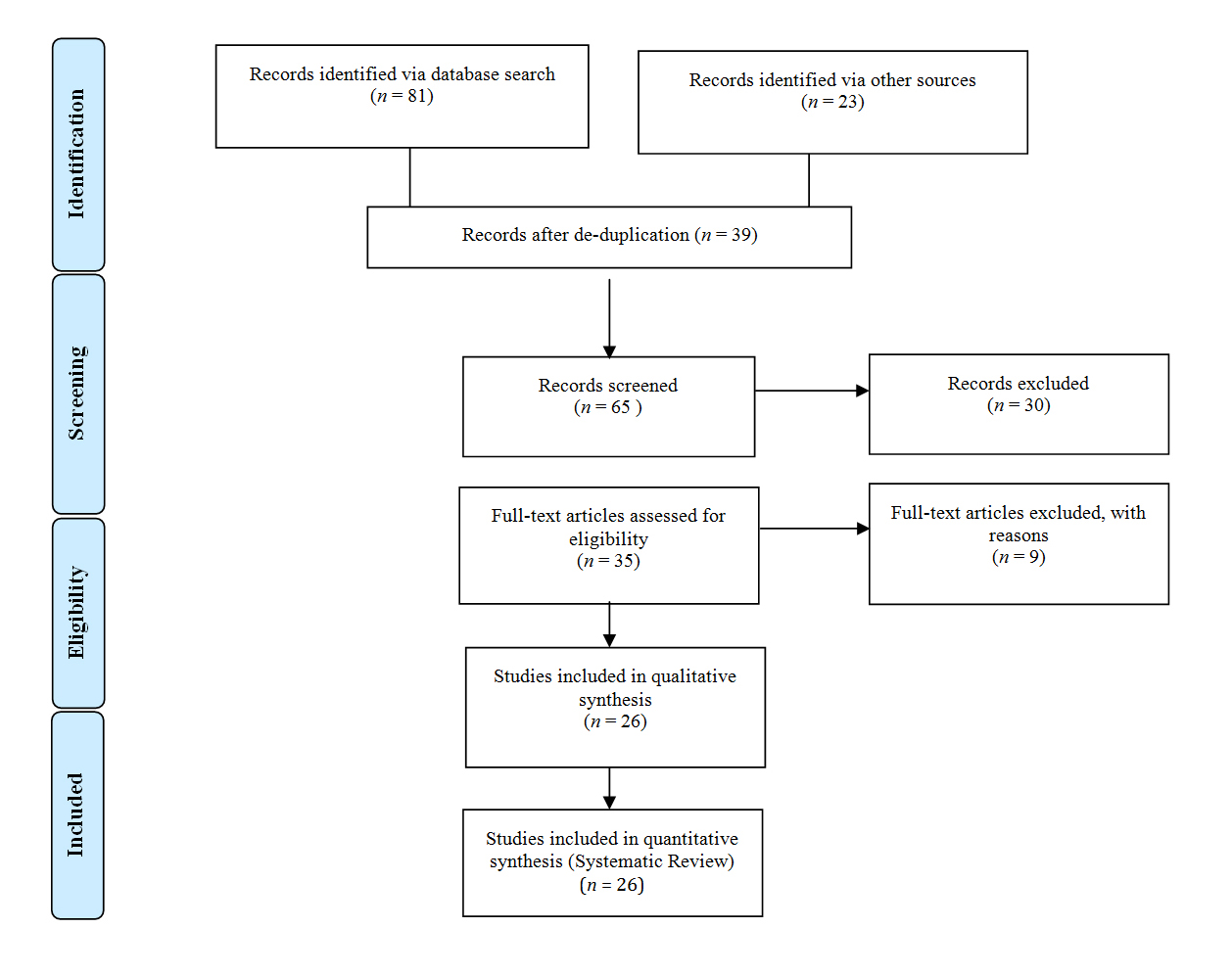 Fig.1 Flow Chart
Fig.1 Flow Chart
Patient inclusion criteria were: (1) either gender; (2) 18 and older; (3) diagnosed with spontaneous coronary dissection; (4) had undergone a non-cardiac surgical procedure; (5) presented with acute coronary syndromes intraoperatively or postoperatively (up to 30 post-intervention); (6) unstable angina as defined by chest pain or ischemic equivalent (pulmonary congestion, cardiogenic shock) at rest and compatible electrocardiographic changes (ST segment depression of at least 0.05 mV or T wave inversion); (7) “acute myocardial infarction” defined as elevation and decrease of myocardial necrosis markers: troponin T or I or CKMB mass associated with ischemic symptoms or associated with electrocardiographic changes compatible with ischemia: changes of the ST segment or T wave or Q wave appearance.
Exclusion criteria were those who had not undergone coronary angiography or patients with SCAD who did not otherwise meet the inclusion criteria, such as patients with unstable angina, but no electrocardiographic abnormalities.
2.3 Sources of informationThe review protocol was based on the literature search criteria using mesh terms in the main databases such as Pubmed, Medline, Bireme, EBSCO, and Scielo. All references are registered in EndNote at site:
http://www.myendnoteweb.com/EndNoteWeb.html?cat=myrefs&.
2.4 Search strategyAn example of a search strategies appear in MEDLINE/Pubmed, Web Of Science, ScienceDirect Journals (Elsevier), Scopus (Elsevier), and OneFile (Gale) and followed these steps: - search for mesh terms (Metalloproteinases, dysplasia fibromuscular, clinical trial Spontaneous Coronary Artery Dissection), use of the bouleanos "and" between mesh terms and "or" among historical findings.
2.5 Statistical treatment of literary findingsA descriptive analysis was performed using standard parameters for mean, standard deviation, and amplitude. An Anderson-Darling normality test (α-level > 0.10 considered "normal") was performed for continuous and categorical data, with a subsequent application of a Kruskal-Wallis analysis of variance to the internal data for each study alone, and deeming a p-value of less than 0.05 as statistically significant. An equivalence test (I2) between the data of each work was also performed.
2.6 Literature review and discussionThe metanalysis provided information about spontaneous coronary artery dissection as a rare, though potentially fatal (50% sudden death) cause of acute myocardial infarction with estimated cineangiography incidence between 0.04% and 0.20% [13]. There were no statistical differences between the studies. The equivalence level between the study results was 93.5%. (Table 1)
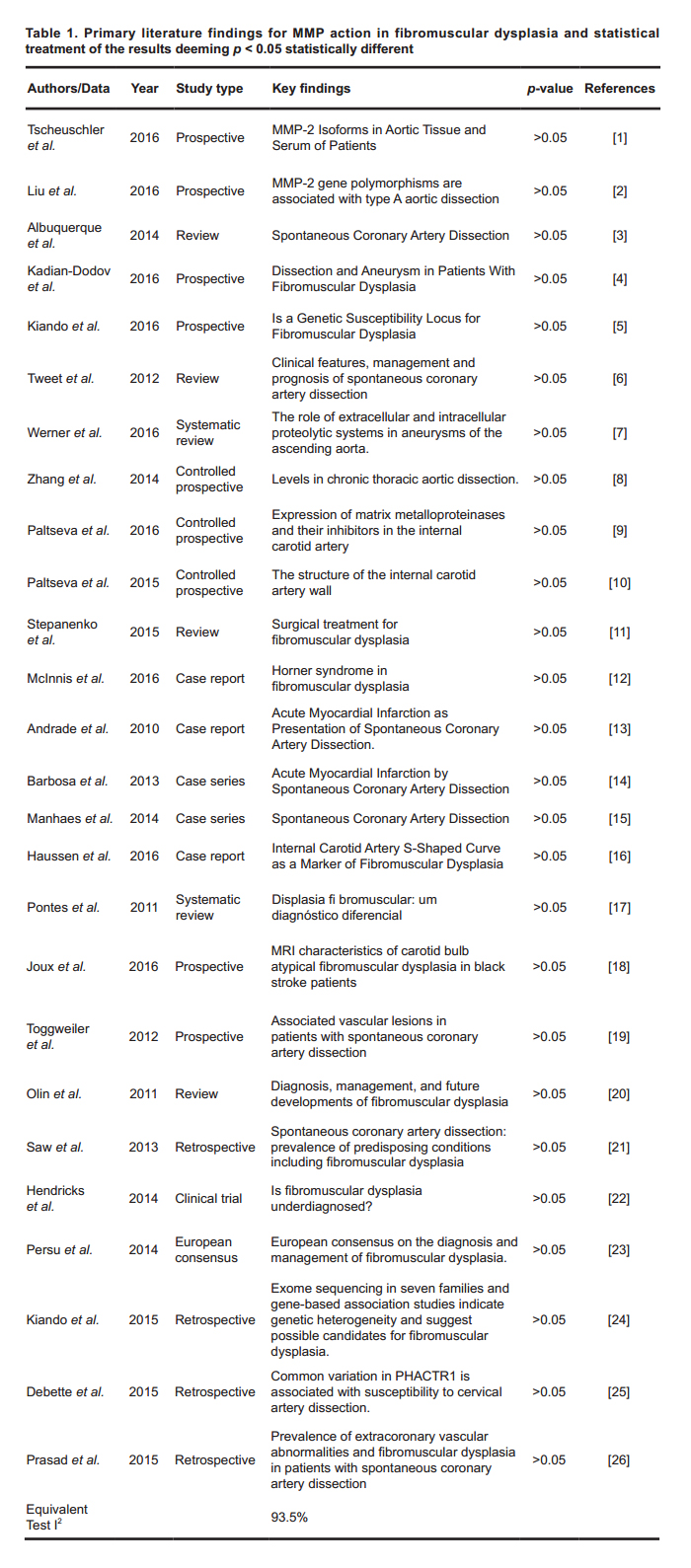 Table 1. Primary literature findings for MMP action in fibromuscular dysplasia and statistical treatment of the results deeming p < 0.05 statistically different
Table 1. Primary literature findings for MMP action in fibromuscular dysplasia and statistical treatment of the results deeming p < 0.05 statistically different
The anterior descending coronary artery is the vessel most affected by SCAD. It has a prevalence of 40–60%. It is followed by the circumflex artery and its branches (30%), primarily the medial and distal segments [14]. The disease may associate with a genetic component as it mostly affects Caucasians with an HLA-DR6 histocompatibility antigen [17].
Pro-MMP-2 was present in all tissue, and serum, samples of all patients with ascending aortic/aortic root aneurysms [1]. Active MMP-2 species are not released into the circulatory system or are undetectable in serum. There is no reliable connection between MMP-2 isoforms in aortic tissue and serum. Nor is there any indication that pro-MMP-2 functions as a major aortic wall stress common marker [1].
MMP-2 plays an important role in the pathogenesis of type A aortic dissection (AD). One study analyzed the association of 3 single nucleotide polymorphisms in the MMP-2 gene with risk of type A (AD) and aortic diameters. MMP-2 polymorphisms contributed to type A susceptibility. MMP-2 gene nucleotides associate with AD size which could be targeted for new drug therapies [2]. MMP tissue inhibitor imbalances, the TIMPs may lead to aortic wall failure. Total MMP-1, total MMP-9, and active MMP-9 levels were higher and total MMP-2 levels were lower in dissection tissue than in control tissue. The ratio of MMP-9 to TIMP-1 and the ratio of active to total MMP-2 were higher. The ratio of MMP-2 to TIMP-2 was lower in dissection tissue. Patients had a higher ratios of plasma-active to total MMP-9 than controls [8]. Age and hypertension associated with increased MMP levels. Several MMPs increased levels and increased MMP-to-TIMP ratios in aortic tissue suggested an environment-favoring proteolysis. This may promote progressive extracellular matrix destruction and medial degeneration after aortic dissection. An elevated active-to-total MMP-9 ratio in plasma may be a biomarker for end-stage aneurysm in patients with chronic thoracic aortic disease [8].
SCAD, at the molecular level, may be related to MMP expression and consequent elastin degradation [5]. Elastic fiber fragmentation in coronary arteries is due to an imbalance between metalloproteinase 2 (MMP2) and metalloproteinase 9 (MMP9) on its inhibitor TIMP1 and TIMP2 [5]. This may be the primary pathological cause and enzymatic homeostasis during treatment. Future studies of MMP effect as a SCAD predictor could be one such approach.
The presence of a common variant, rs9349379, located on chromosome 6 of the phosphatase and actin-regulator gene 1 (PHACTR1), has been shown to increase foot-and-mouth disease (FMD) risk by about 40% [5]. rs9349379 correlates with PHACTR1 expression in fibroblasts of patients with FMD and controls. The presence of this allele also increases FD risk and is present with cervical artery dissection and migraine risk. It is often reported in FD patients. The PHACTR1 role in maintaining vascular vessel integrity is not fully understood [5,24–26].
Generally, diagnosis is performed by "catheterism". An intramural hematoma is difficult to detect visually. Diagnoses may be imprecise. Other diagnostic technologies, such as coronary computed tomography and intravascular ultrasound are used. Symptomatology depends on which coronaries vessels suffered dissection and how dissected they are. Patients may present asymptomatic [2,3].
Half of the survivors had survival rates of approximately 80.0% at 30 months. Half developed a second dissection within two months [13]. Women had lower survival rates than men particularly when the event occurred outside peripartum [13].
Some studies have tested the hypothesis of a relationship between SCAD and the presence of FD in other arterial sites. Some researchers performed whole-body angio-CT and angio-MRI on SCAD patients on three with cases of renal FD [3,19]. Low FD incidence is related to poor imaging method sensitivity which detects stenosis in less than 50.0% of the middle and distal arterial segments [3].
A 50.0% prevalence of FD in the external iliac artery of 16 patients with SCAD undergoing iliofemoral angiography was found in one study [6]. Another found 86% of 50 patients with SCAD had with FD [21]. A study of family members of SCAD patients found that only 7.0% did.
A study of 144 patients reported on treatment and follow-up for fibromuscular dysplasia [11]. Post-carotid surgery follow-up did not show cardiac arrest, stenosis, or death. Persistent normalization of blood pressure was achieved in 11 (73.3%) cases. Surgical treatment with some forms of FD provides satisfactory results if the recommended strategy is followed [11].
Between 2008 and 2010, 5 patients hospitalized with acute coronary syndrome, as evidenced via coronary angiography, suffered spontaneous coronary dissection. Intracoronary ultrasonography was useful in diagnosing spontaneous coronary dissection and in guiding percutaneous treatment [14,26].
A retrospective unicentric study provided corroboration by identifying 25 patients with spontaneous coronary artery dissection, 56.0% of whom were females, aged 48.8 ± 10. In 92.0% of the cases, acute coronary syndrome was present. A conservative strategy was performed in 56%, percutaneous coronary intervention in 40%, and myocardial revascularization in 4%, of the cases. The existence of a variety of therapeutic strategies confirms the still-unsettled opinion as to the ideal approach to spontaneous coronary artery dissection and an emphasis on individualized treatment [15,22,23].
The patient was diagnosed with this pathology due to a prior episode of acute myocardial infarction and the presence of coronary tortuosity, which are SCAD predictors. After being treated as described above, the patient remained asymptomatic.
We intend a follow-up study of MMPs as predictors of spontaneous coronary artery dissection.
•
•
•
•
•
The work was supported by Domingo Braile Institute - São José do Rio Preto - SP, Brazil.
The authors declare no conflicts of interest.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
Sabino SB, Sternieri GB, Braile-Sternieri MCVB, Mustafa EM, Ferreira VRR, Faria LAB, Sbardellini BC, Queiroz COV, Braile DM, Ramirez AVG, Filho IJZ, Cornélio ML. Metalloproteinases and Spontaneous Coronary Artery Dissection Relationships: A Systematic Review. Med One. 2018 Jun 30; 3: e180005. https://doi.org/10.20900/mo.20180005

Copyright © 2020 Hapres Co., Ltd. Privacy Policy | Terms and Conditions




